

Analysis of National Trends in Admissions for Pulmonary Embolism
- PMID: 26905364
- PMCID: PMC6026254
- DOI: 10.1016/j.chest.2016.02.638
Analysis of National Trends in Admissions for Pulmonary Embolism
Abstract
Background: Pulmonary embolism (PE) remains a significant cause of hospital admission and health-care costs. Estimates of PE incidence came from the 1990s, and data are limited to describe trends in hospital admissions for PE over the past decade.
Methods: We analyzed Nationwide Inpatient Sample data from 1993 to 2012 to identify patients admitted with PE. We included admissions with International Classification of Diseases, 9th revision, codes listing PE as the principal diagnosis as well as admissions with PE listed secondary to principal diagnoses of respiratory failure or DVT. Massive PE was defined by mechanical ventilation, vasopressors, or nonseptic shock. Outcomes included hospital lengths of stay, adjusted charges, and all-cause hospital mortality. Linear regression was used to analyze changes over time.
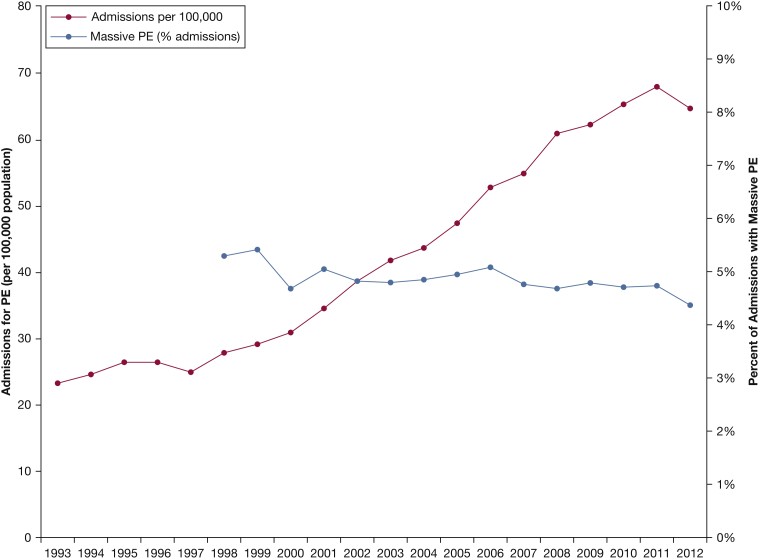
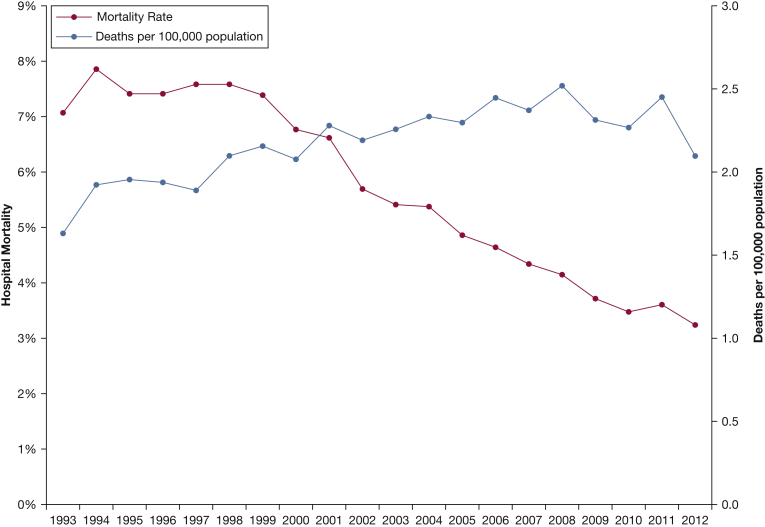
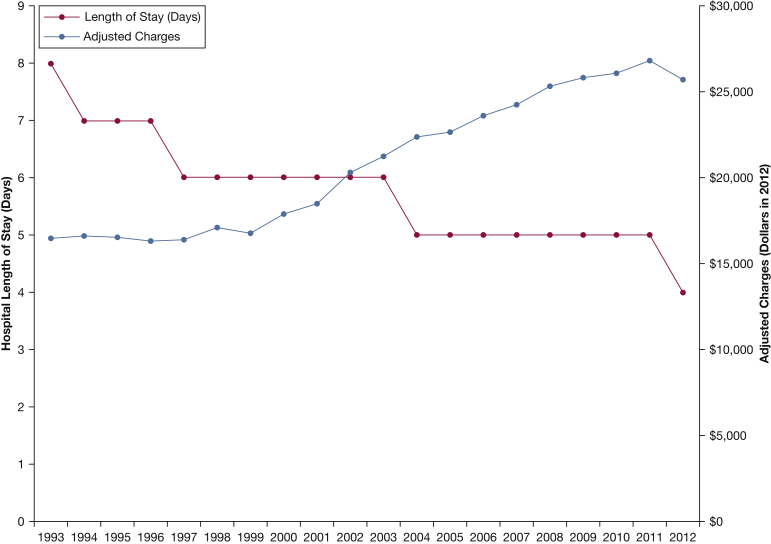
Results: Admissions for PE increased from 23 per 100,000 in 1993 to 65 per 100,000 in 2012 (P < .001). The percent of admissions meeting criteria for massive PE decreased (5.3% to 4.4%, P = .002), but the absolute number of admissions for massive PE increased (from 1.5 to 2.8 per 100,000, P < .001). Median length of stay decreased from 8 (interquartile range [IQR], 6-11) to 4 (IQR, 3-6) days (P < .001). Adjusted hospital charges increased from $16,475 (IQR, $10,748-$26,211) in 1993 to $25,728 (IQR, $15,505-$44,493) in 2012 (P < .001). All-cause hospital mortality decreased from 7.1% to 3.2% (P < .001), but population-adjusted deaths during admission for PE increased from 1.6 to 2.1 per 100,000 (P < .001).
Conclusions: Total admissions and hospital charges for PE have increased over the past two decades. However, the population-adjusted admission rate has increased disproportionately to the incidence of patients with severe PE. We hypothesize that these findings reflect a concerning national movement toward more admissions of less severe PE.
Keywords: hospitalization; mortality; pulmonary embolism.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Analysis of National Trends in Admissions for Pulmonary Embolism.Chest. 2016 Jul;150(1):250. doi: 10.1016/j.chest.2016.04.024. Chest. 2016. PMID: 27396781 No abstract available.
-
Response.Chest. 2016 Jul;150(1):250-1. doi: 10.1016/j.chest.2016.04.023. Chest. 2016. PMID: 27396782 No abstract available.
-
Considerations for the Interpretation of the Results Described in "Analysis of National Trends in Admissions for Pulmonary Embolism".Chest. 2016 Aug;150(2):467. doi: 10.1016/j.chest.2016.03.064. Chest. 2016. PMID: 27502981 No abstract available.
References
-
- Geske J.B., Smith S.B., Morgenthaler T.I., Mankad S.V. Care of patients with acute pulmonary emboli: a clinical review with cardiovascular focus. Expert Rev Cardiovasc Ther. 2012;10(2):235–250. - PubMed
-
- Silverstein M.D., Heit J.A., Mohr D.N., Petterson T.M., O’Fallon W.M., Melton L.J., 3rd. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158(6):585–593. - PubMed
-
- Stein P.D., Dalen J.E., Matta F. Underuse of vena cava filters in unstable patients with acute pulmonary embolism. Am J Med. 2014;127(11):6. - PubMed
-
- Stein P.D., Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465–470. - PubMed
-
- Stein P.D., Matta F. Vena cava filters in unstable elderly patients with acute pulmonary embolism. Am J Med. 2014;127(3):222–225. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
