

Aortic Neck Anatomic Features and Predictors of Outcomes in Endovascular Repair of Abdominal Aortic Aneurysms Following vs Not Following Instructions for Use
- PMID: 26905372
- PMCID: PMC4966526
- DOI: 10.1016/j.jamcollsurg.2015.12.037
Aortic Neck Anatomic Features and Predictors of Outcomes in Endovascular Repair of Abdominal Aortic Aneurysms Following vs Not Following Instructions for Use
Abstract
Background: A significant number of patients undergo endovascular repair of abdominal aortic aneurysms (EVAR) outside the instructions for use (IFU). This study will examine various aortic neck features and their predictors of clinical outcomes.
Study design: We performed a retrospective analysis of prospectively collected data on EVAR patients. Neck features outside IFU were analyzed. Kaplan-Meier and multivariate analyses were used to predict their effect as single features, or in combination, on outcomes.
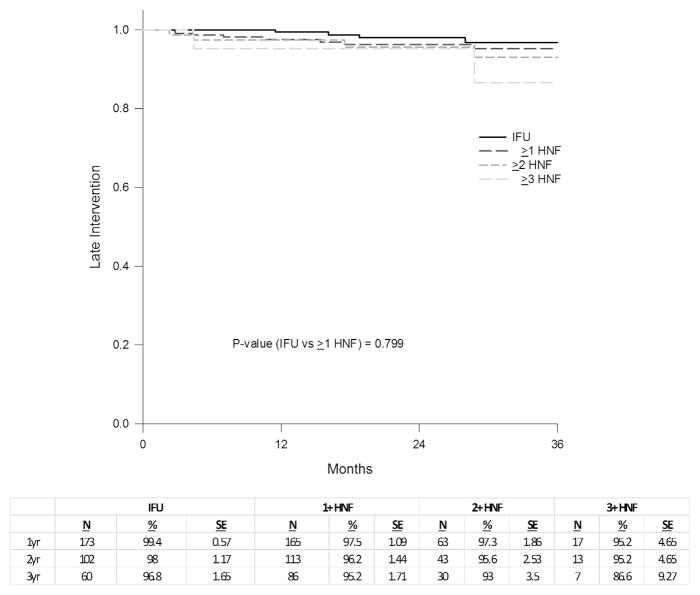
Results: Fifty-two percent of 526 patients had 1 or more features outside the IFU. The overall technical success rate was 99%, and perioperative complication rates were 7% and 12% for IFU vs outside IFU use, respectively (p = 0.04). Type I early endoleak and early intervention rates were 7% and 10% for IFU vs 18% and 24% for outside IFU (p = 0.0002 and p < 0.0001). At a mean follow-up of 30 months, freedom from late type I endoleak and late reintervention at 1, 2, and 3 years for IFU were 99.5%, 99.5%, and 98.4%, and 99.4%, 98%, and 96.8%; vs 98.9%, 98.1%, and 98.1%, and 97.5%, 96.2%, and 95.2% for outside IFU (p = 0.049 and 0.799), respectively. Survival rates at 1, 2, and 3 years for IFU were 97%, 93.5%, and 89.8%; vs 93.7%, 88.8%, and 86.3% for outside IFU (p = 0.035). Multivariate analysis showed that a neck angle > 60 degrees had odds ratios for death, sac expansion, and early intervention of 6, 2.6, and 3.3, respectively; neck length < 10 mm had odds ratios of 2.8 for deaths, 3.4 for early intervention, 4.6 for late reintervention, and 4.3 for late type I endoleak.
Conclusions: Patients with neck features outside IFU can be treated with EVAR; however, they have higher rates of early and late type I endoleak, early intervention, and late death.
Copyright © 2016 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures



Comment in
-
Discussion.J Am Coll Surg. 2016 Apr;222(4):589-90. doi: 10.1016/j.jamcollsurg.2016.01.021. J Am Coll Surg. 2016. PMID: 27016986 No abstract available.
References
-
- Aburahma AF, Campbell JE, Mousa AY, et al. Clinical outcomes for hostile versus favorable aortic neck anatomy in endovascular aortic aneurysm repair using modular devices. J Vasc Surg. 2011;54:13–21. - PubMed
-
- Antoniou GA, Georgiadis GS, Antoniou SA, et al. A meta-analysis of outcomes of endovascular abdominal aortic aneurysm repair in patients with hostile and friendly neck anatomy. J Vasc Surg. 2013;57:527–538. - PubMed
-
- Stather PW, Wild JB, Sayers RD, et al. Endovascular aortic aneurysm repair in patients with hostile neck anatomy. J Endovasc Ther. 2013;20:623–637. - PubMed
-
- Stather PW, Sayers RD, Cheah A, et al. Outcomes of endovascular aneurysm repair in patients with hostile neck anatomy. Eur J Vasc Endovasc Surg. 2012;44:556–561. - PubMed
-
- Hager ES, Cho JS, Makaroun MS, et al. Endografts with suprarenal fixatiion do not perform better than those with infrarenal fixation in the treatment of patients with short straight proximal aortic necks. J Vasc Surg. 2015;55:1242–1246. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
