

High-Dose Perioperative Atorvastatin and Acute Kidney Injury Following Cardiac Surgery: A Randomized Clinical Trial
- PMID: 26906014
- PMCID: PMC4843765
- DOI: 10.1001/jama.2016.0548
High-Dose Perioperative Atorvastatin and Acute Kidney Injury Following Cardiac Surgery: A Randomized Clinical Trial
Abstract
Importance: Statins affect several mechanisms underlying acute kidney injury (AKI).
Objective: To test the hypothesis that short-term high-dose perioperative atorvastatin would reduce AKI following cardiac surgery.
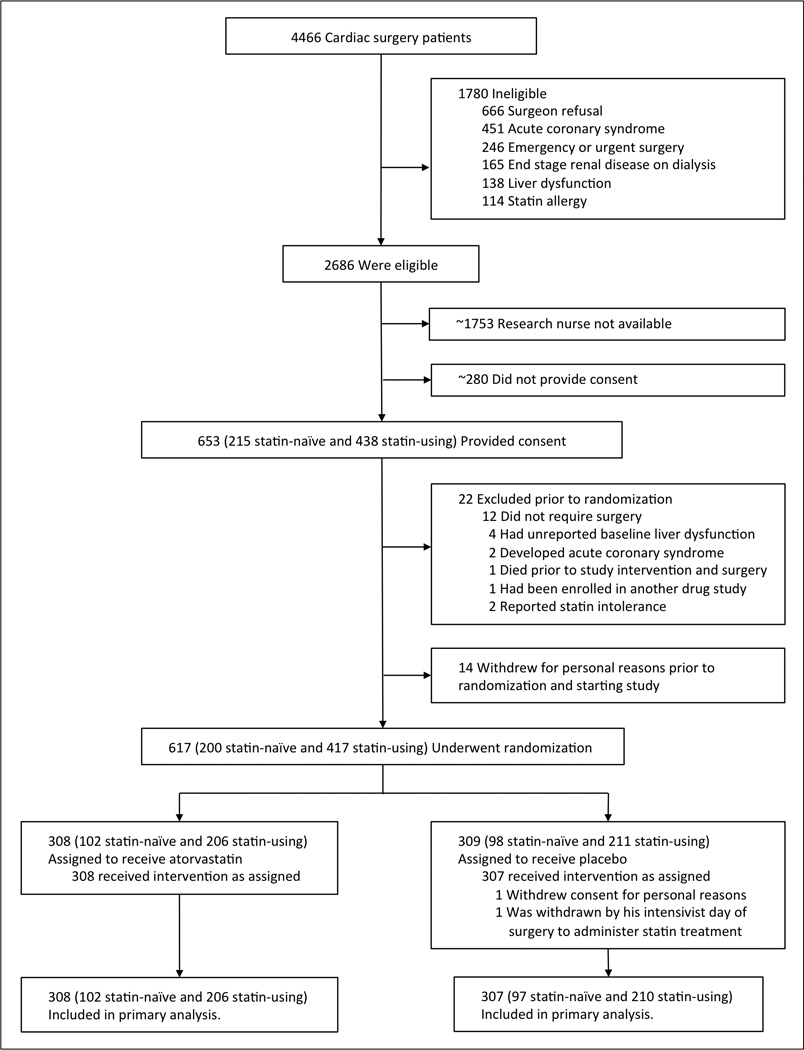
Design, setting, and participants: Double-blinded, placebo-controlled, randomized clinical trial of adult cardiac surgery patients conducted from November 2009 to October 2014 at Vanderbilt University Medical Center.
Interventions: Patients naive to statin treatment (n = 199) were randomly assigned 80 mg of atorvastatin the day before surgery, 40 mg of atorvastatin the morning of surgery, and 40 mg of atorvastatin daily following surgery (n = 102) or matching placebo (n = 97). Patients already taking a statin prior to study enrollment (n = 416) continued taking the preenrollment statin until the day of surgery, were randomly assigned 80 mg of atorvastatin the morning of surgery and 40 mg of atorvastatin the morning after (n = 206) or matching placebo (n = 210), and resumed taking the previously prescribed statin on postoperative day 2.
Main outcomes and measures: Acute kidney injury defined as an increase of 0.3 mg/dL in serum creatinine concentration within 48 hours of surgery (Acute Kidney Injury Network criteria).
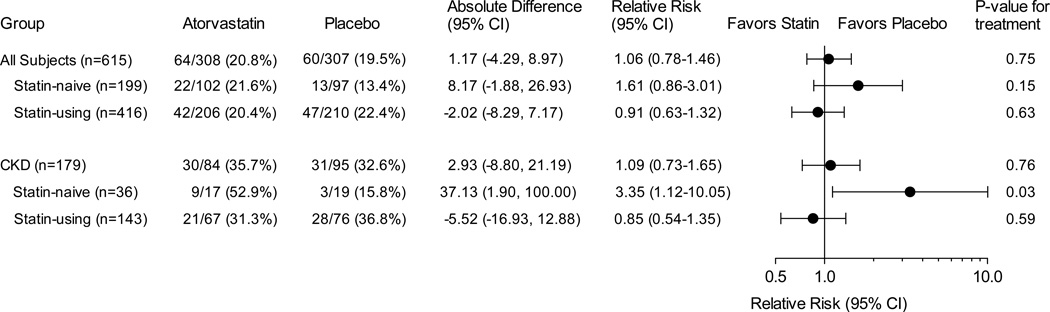
Results: The data and safety monitoring board recommended stopping the group naive to statin treatment due to increased AKI among these participants with chronic kidney disease (estimated glomerular filtration rate <60 mL/min/1.73 m2) receiving atorvastatin. The board later recommended stopping for futility after 615 participants (median age, 67 years; 188 [30.6%] were women; 202 [32.8%] had diabetes) completed the study. Among all participants (n = 615), AKI occurred in 64 of 308 (20.8%) in the atorvastatin group vs 60 of 307 (19.5%) in the placebo group (relative risk [RR], 1.06 [95% CI, 0.78 to 1.46]; P = .75). Among patients naive to statin treatment (n = 199), AKI occurred in 22 of 102 (21.6%) in the atorvastatin group vs 13 of 97 (13.4%) in the placebo group (RR, 1.61 [0.86 to 3.01]; P = .15) and serum creatinine concentration increased by a median of 0.11 mg/dL (10th-90th percentile, -0.11 to 0.56 mg/dL) in the atorvastatin group vs by a median of 0.05 mg/dL (10th-90th percentile, -0.12 to 0.33 mg/dL) in the placebo group (mean difference, 0.08 mg/dL [95% CI, 0.01 to 0.15 mg/dL]; P = .007). Among patients already taking a statin (n = 416), AKI occurred in 42 of 206 (20.4%) in the atorvastatin group vs 47 of 210 (22.4%) in the placebo group (RR, 0.91 [0.63 to 1.32]; P = .63).
Conclusions and relevance: Among patients undergoing cardiac surgery, high-dose perioperative atorvastatin treatment compared with placebo did not reduce the risk of AKI overall, among patients naive to treatment with statins, or in patients already taking a statin. These results do not support the initiation of statin therapy to prevent AKI following cardiac surgery.
Trial registration: clinicaltrials.gov Identifier: NCT00791648.
Conflict of interest statement
Potential conflicts of interest:
No author reports any relevant conflicts of interest.
Figures
Comment in
-
Perioperative Statins in Cardiac Surgery and Acute Kidney Injury.JAMA. 2016 Mar 1;315(9):873-4. doi: 10.1001/jama.2016.0245. JAMA. 2016. PMID: 26905755 No abstract available.
-
Statins and acute kidney injury following cardiac surgery: has the last word been told?J Thorac Dis. 2016 Jun;8(6):E451-4. doi: 10.21037/jtd.2016.04.34. J Thorac Dis. 2016. PMID: 27294251 Free PMC article. No abstract available.
-
Statins to Reduce Acute Kidney Injury After Cardiac Surgery.JAMA. 2016 Jul 19;316(3):349. doi: 10.1001/jama.2016.6134. JAMA. 2016. PMID: 27434455 No abstract available.
-
Statins to Reduce Acute Kidney Injury After Cardiac Surgery--Reply.JAMA. 2016 Jul 19;316(3):349-50. doi: 10.1001/jama.2016.6148. JAMA. 2016. PMID: 27434456 No abstract available.
-
No recommendation of routine perioperative statin use for prevention of acute kidney injury in patients undergoing cardiac surgery.J Thorac Dis. 2016 Jul;8(7):E618-20. doi: 10.21037/jtd.2016.05.45. J Thorac Dis. 2016. PMID: 27500739 Free PMC article. No abstract available.
-
Ameliorating acute kidney injury following cardiac surgery: do high dose perioperative statins play a role?J Thorac Dis. 2016 Aug;8(8):1883-5. doi: 10.21037/jtd.2016.06.42. J Thorac Dis. 2016. PMID: 27618995 Free PMC article. No abstract available.
-
Does high-dose perioperative use of statins ameliorate acute kidney injury following cardiac surgery?J Thorac Dis. 2016 Oct;8(10):E1235-E1237. doi: 10.21037/jtd.2016.10.22. J Thorac Dis. 2016. PMID: 27867596 Free PMC article. No abstract available.
References
-
- Rosner MH, Okusa MD. Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol. 2006;1:19–32. - PubMed
-
- Cooper WA, O’Brien SM, Thourani VH, et al. Impact of renal dysfunction on outcomes of coronary artery bypass surgery: results from the Society of Thoracic Surgeons National Adult Cardiac Database. Circulation. 2006;113(8):1063–1070. - PubMed
-
- Swaminathan M, Shaw AD, Phillips-Bute BG, et al. Trends in acute renal failure associated with coronary artery bypass graft surgery in the United States. Crit Care Med. 2007;35:2286–2291. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
