

Nanotechnology in diagnosis and treatment of coronary artery disease
- PMID: 26906471
- PMCID: PMC4794112
- DOI: 10.2217/nnm.16.3
Nanotechnology in diagnosis and treatment of coronary artery disease
Abstract
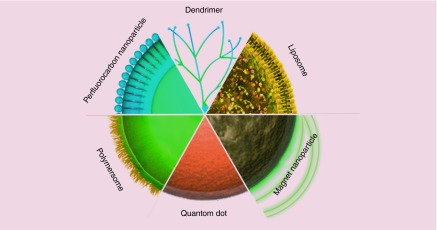
Nanotechnology could provide a new complementary approach to treat coronary artery disease (CAD) which is now one of the biggest killers in the Western world. The course of events, which leads to atherosclerosis and CAD, involves many biological factors and cellular disease processes which may be mitigated by therapeutic methods enhanced by nanotechnology. Nanoparticles can provide a variety of delivery systems for cargoes such as drugs and genes that can address many problems within the arteries. In order to improve the performance of current stents, nanotechnology provides different nanomaterial coatings, in addition to controlled-release nanocarriers, to prevent in-stent restenosis. Nanotechnology can increase the efficiency of drugs, improve local and systematic delivery to atherosclerotic plaques and reduce the inflammatory or angiogenic response after intravascular intervention. Nanocarriers have potential for delivery of imaging and diagnostic agents to precisely targeted destinations. This review paper will cover the current applications and future outlook of nanotechnology, as well as the main diagnostic methods, in the treatment of CAD.
Keywords: atherosclerosis; coronary artery disease; nanocarriers; nanotechnology; restenosis; stent coatings; vulnerable plaque.
Conflict of interest statement
Financial & competing interests disclosure MR Hamblin was supported by US NIH Grant R01AI050875. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- Badimon L, Vilahur G. Thrombosis formation on atherosclerotic lesions and plaque rupture. J. Intern. Med. 2014;276(6):618–632. - PubMed
-
- Cominacini L, Garbin U, Mozzini C, et al. The atherosclerotic plaque vulnerability: focus on the oxidative and endoplasmic reticulum stress in orchestrating the macrophage apoptosis in the formation of the necrotic core. Curr. Med. Chem. 2015;22(13):1565–1572. - PubMed
-
- Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient a call for new definitions and risk assessment strategies: part I. Circulation. 2003;108(14):1664–1672. - PubMed
-
- Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature. 2011;473:317–325. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous