

High prevalence of secondary factors for bone fragility in patients with a recent fracture independently of BMD
- PMID: 26906974
- PMCID: PMC4764633
- DOI: 10.1007/s11657-016-0258-3
High prevalence of secondary factors for bone fragility in patients with a recent fracture independently of BMD
Abstract
In this study, we demonstrate a high prevalence of secondary factors in patients with a recent fracture independently of bone mineral density (BMD). Our results suggest that patients with a recent fracture should be screened for secondary factors for bone fragility regardless of BMD values.
Introduction: Secondary factors for bone fragility are common in patients with osteoporosis who have sustained a fracture. The majority of fragility fractures occurs, however, in patients with osteopenia, and it is not known whether secondary factors may contribute to fracture risk in these patients or in those with normal BMD.
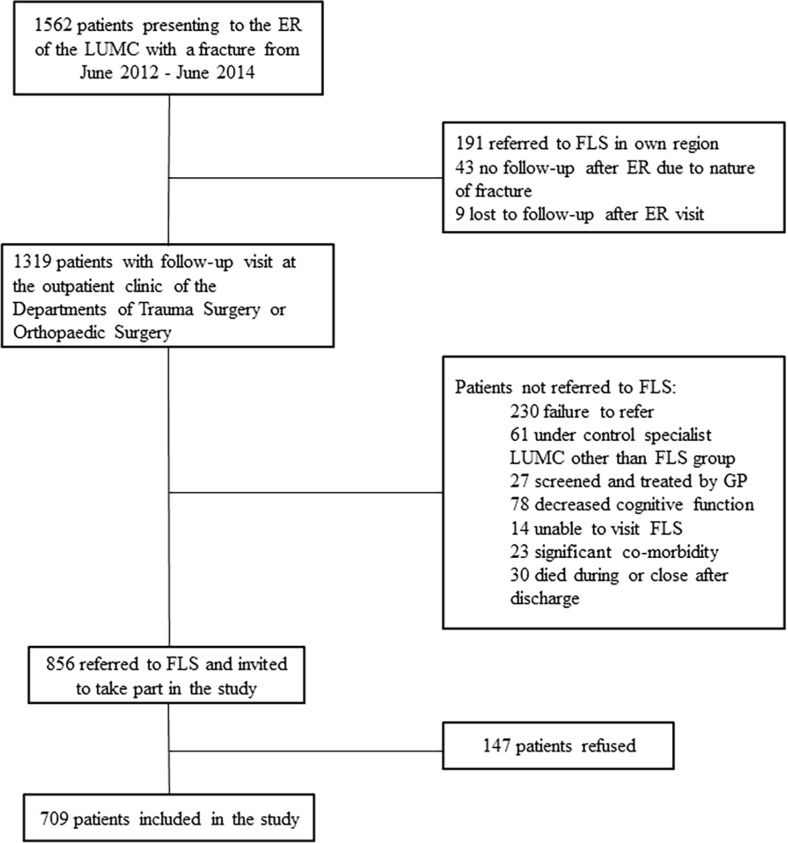
Methods: Prospective cohort study evaluating the prevalence of secondary factors for bone fragility in consecutive patients referred to our fracture liaison service from June 2012 to June 2014 after a recent fracture.
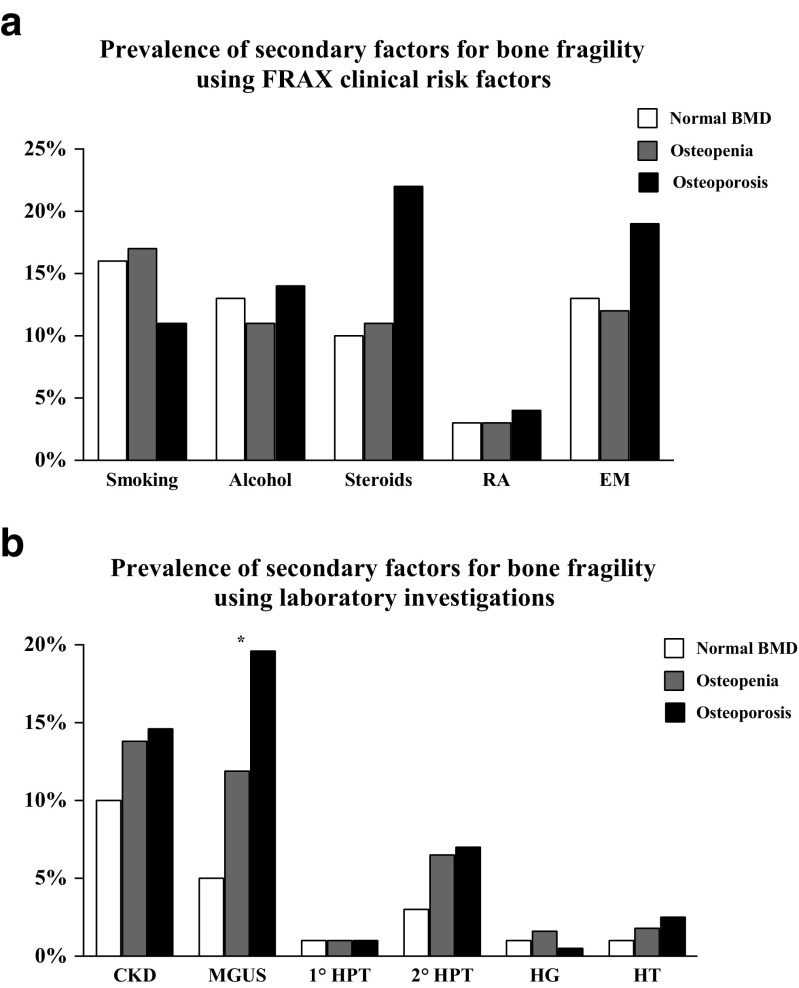
Results: Seven hundred nine patients were included, 201 (28 %) with osteoporosis, 391 (55 %) with osteopenia and 117 (17 %) with normal BMD. Mean age was 66.0 ± 9.8 years, 504 (73 %) were women and 390 (57 %) had one or more underlying secondary factor. Evaluation of clinical risk factors using fracture risk assessment tool (FRAX) identified 38 % of patients with ≥1 secondary factor including smoking (18 %), excessive alcohol use (12 %), glucocorticoid use (12 %) and rheumatoid arthritis (3 %). Laboratory investigations revealed chronic kidney disease in 13 %, monoclonal gammopathy also in 13 % and primary or secondary hyperparathyroidism in 1 and 6 %, respectively. Secondary factors for bone fragility were equally prevalent in patients with osteoporosis, osteopenia or normal BMD.
Conclusions: Our findings demonstrate a high prevalence of secondary factors for bone fragility in patients who have sustained a recent fracture, independently of BMD. The significant number of documented factors, which were treatable, suggest that patients who sustained a fracture should be screened for secondary factors for bone fragility regardless of BMD values to optimise secondary fracture prevention.
Keywords: Fracture liaison service; Fragility fracture; Osteopenia; Osteoporosis; Secondary factors.
Conflict of interest statement
Compliance with ethical standards Conflicts of interest None
Figures
References
-
- Tosteson AN, Burge RT, Marshall DA, Lindsay R. Therapies for treatment of osteoporosis in US women: cost-effectiveness and budget impact considerations. Am J Manag Care. 2008;14:605–615. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
