

A novel and accurate predictor of survival for patients with hepatocellular carcinoma after surgical resection: the neutrophil to lymphocyte ratio (NLR) combined with the aspartate aminotransferase/platelet count ratio index (APRI)
- PMID: 26907597
- PMCID: PMC4763424
- DOI: 10.1186/s12885-016-2189-1
A novel and accurate predictor of survival for patients with hepatocellular carcinoma after surgical resection: the neutrophil to lymphocyte ratio (NLR) combined with the aspartate aminotransferase/platelet count ratio index (APRI)
Abstract
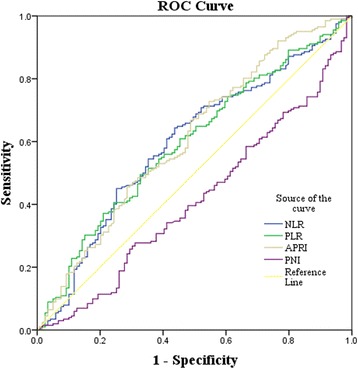
Background: The occurrence and development of hepatocellular carcinoma (HCC) depends largely on such non-tumor factors as inflammatory condition, immune state, viral infection and liver fibrosis. Various inflammation-based prognostic scores have been associated with survival in patients with HCC, such as the neutrophil/lymphocyte ratio (NLR), the platelet/lymphocyte ratio (PLR) and the prognostic nutritional index (PNI). The aspartate aminotransferase/platelet count ratio index (APRI) is thought to be a biomarker of liver fibrosis and cirrhosis. This study aims to evaluate the ability of these indices to predict survival in HCC patients after curative hepatectomy, and probe the increased prognostic accuracy of APRI combined with established inflammation-based prognostic scores.
Methods: Data were collected retrospectively from 321 patients who underwent curative resection for HCC. Preoperative NLR, PLR, PNI, APRI and clinico-pathological variables were analyzed. Univariate and multivariate analyses were performed to identify the predictive value of the above factors for disease-free survival (DFS) and overall survival (OS).
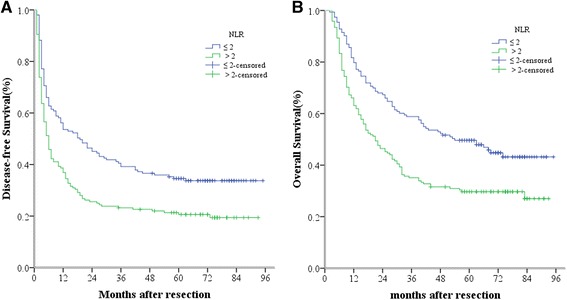
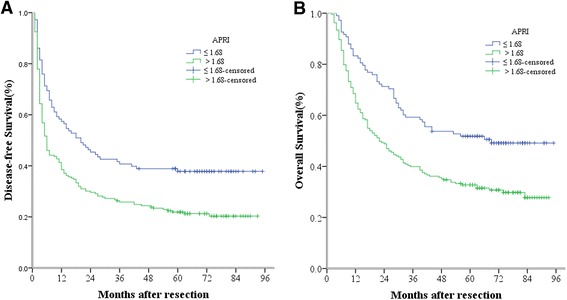
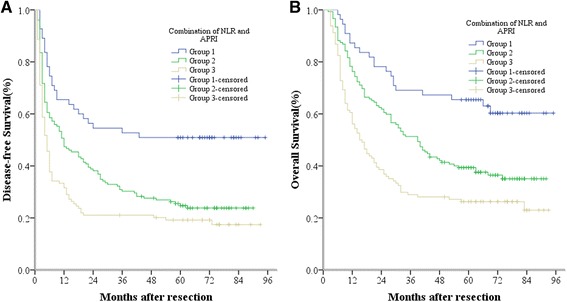
Results: Univariate analysis showed that NLR, PLR, PNI and APRI were significantly associated with DFS and OS in HCC patients with curative resection. Multivariate analysis showed that NLR and APRI were superior to PLR and PNI, and both were independently correlated with DFS and OS. Preoperative NLR >2 or APRI >1.68 predicted poor prognosis of patients with HCC after hepatectomy. Furthermore, the predictive range of NLR combined with APRI was more sensitive than that of either measure alone.
Conclusions: Preoperative NLR and APRI are independent predictors of DFS and OS in patients with HCC after surgical resection. Higher levels of NLR or APRI predict poorer outcomes in HCC patients. Intriguingly, combining NLR and APRI increases the prognostic accuracy of testing.
Figures
Similar articles
-
Prognostic significance of preoperative aspartate aminotransferase to neutrophil ratio index in patients with hepatocellular carcinoma after hepatic resection.Oncotarget. 2016 Nov 1;7(44):72276-72289. doi: 10.18632/oncotarget.10848. Oncotarget. 2016. PMID: 27472390 Free PMC article.
-
Preoperative aspartate aminotransferase to platelet ratio is an independent prognostic factor for hepatitis B-induced hepatocellular carcinoma after hepatic resection.Ann Surg Oncol. 2014 Nov;21(12):3802-9. doi: 10.1245/s10434-014-3771-x. Epub 2014 May 22. Ann Surg Oncol. 2014. PMID: 24849520
-
Inflammation scores predict the survival of patients with hepatocellular carcinoma who were treated with transarterial chemoembolization and recombinant human type-5 adenovirus H101.PLoS One. 2017 Mar 29;12(3):e0174769. doi: 10.1371/journal.pone.0174769. eCollection 2017. PLoS One. 2017. PMID: 28355305 Free PMC article.
-
Prognostic value of neutrophil-to-lymphocyte ratio in patients with hepatocellular carcinoma receiving curative therapies: a systematic review and meta-analysis.BMC Cancer. 2025 Mar 29;25(1):571. doi: 10.1186/s12885-025-13972-w. BMC Cancer. 2025. PMID: 40158082 Free PMC article.
-
Prognostic and predictive value of neutrophil-to-lymphocyte ratio after curative rectal cancer resection: A systematic review and meta-analysis.Surg Oncol. 2021 Jun;37:101556. doi: 10.1016/j.suronc.2021.101556. Epub 2021 Mar 31. Surg Oncol. 2021. PMID: 33819850
Cited by
-
Association of blood neutrophil lymphocyte ratio in the patients with postmenopausal osteoporosis.Pak J Med Sci. 2016 May-Jun;32(3):762-5. doi: 10.12669/pjms.323.10292. Pak J Med Sci. 2016. PMID: 27375729 Free PMC article.
-
Combination of Preoperative Circulating Tumor Cell Count and Neutrophil-Lymphocyte Ratio for Prognostic Prediction in Hepatocellular Carcinoma Patients after Curative Hepatectomy.Biomed Res Int. 2022 Jul 16;2022:7305953. doi: 10.1155/2022/7305953. eCollection 2022. Biomed Res Int. 2022. PMID: 35880030 Free PMC article.
-
The lymphocyte-to-monocyte ratio is a superior predictor of overall survival compared to established biomarkers in HCC patients undergoing liver resection.Sci Rep. 2018 Feb 7;8(1):2535. doi: 10.1038/s41598-018-20199-2. Sci Rep. 2018. PMID: 29416061 Free PMC article.
-
Neutrophil-To-Lymphocyte and Platelet-To-Lymphocyte Ratios as Prognostic Markers of Survival in Patients with Head and Neck Tumours-Results of a Retrospective Multicentric Study.Int J Environ Res Public Health. 2020 Mar 7;17(5):1742. doi: 10.3390/ijerph17051742. Int J Environ Res Public Health. 2020. PMID: 32155982 Free PMC article.
-
Nomogram for predicting early cancer-related death due to recurrence after liver resection in hepatocellular carcinoma patients with Barcelona Clinic Liver Cancer (BCLC) stage B/C: a multicenter study.BMC Gastroenterol. 2025 Jan 12;25(1):14. doi: 10.1186/s12876-025-03588-6. BMC Gastroenterol. 2025. PMID: 39800706 Free PMC article.
References
-
- Mano Y, Shirabe K, Yamashita Y-i, Harimoto N, Tsujita E, Takeishi K, et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival after hepatectomy for hepatocellular carcinoma: a retrospective analysis. Ann Surg. 2013;258(2):301–305. doi: 10.1097/SLA.0b013e318297ad6b. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
