

Acquisition of a CD19-negative myeloid phenotype allows immune escape of MLL-rearranged B-ALL from CD19 CAR-T-cell therapy
- PMID: 26907630
- PMCID: PMC4874221
- DOI: 10.1182/blood-2015-08-665547
Acquisition of a CD19-negative myeloid phenotype allows immune escape of MLL-rearranged B-ALL from CD19 CAR-T-cell therapy
Abstract
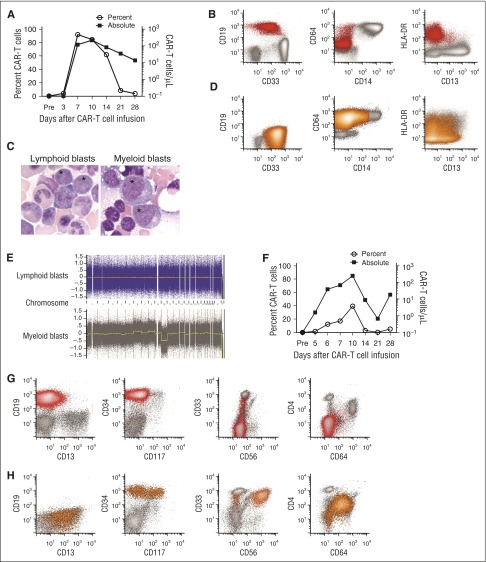
Administration of lymphodepletion chemotherapy followed by CD19-specific chimeric antigen receptor (CAR)-modified T cells is a remarkably effective approach to treating patients with relapsed and refractory CD19(+) B-cell malignancies. We treated 7 patients with B-cell acute lymphoblastic leukemia (B-ALL) harboring rearrangement of the mixed lineage leukemia (MLL) gene with CD19 CAR-T cells. All patients achieved complete remission (CR) in the bone marrow by flow cytometry after CD19 CAR-T-cell therapy; however, within 1 month of CAR-T-cell infusion, 2 of the patients developed acute myeloid leukemia (AML) that was clonally related to their B-ALL, a novel mechanism of CD19-negative immune escape. These reports have implications for the management of patients with relapsed and refractory MLL-B-ALL who receive CD19 CAR-T-cell therapy.
Trial registration: ClinicalTrials.gov NCT02028455.
© 2016 by The American Society of Hematology.
Figures
Comment in
-
Myeloid leukemia switch as immune escape from CD19 chimeric antigen receptor (CAR) therapy.Transl Cancer Res. 2016 Aug;5(Suppl 2):S221-S225. doi: 10.21037/tcr.2016.08.15. Transl Cancer Res. 2016. PMID: 28824851 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
