

Prevalence and risk factors of hypotension associated with preload-dependence during intermittent hemodialysis in critically ill patients
- PMID: 26907782
- PMCID: PMC4765055
- DOI: 10.1186/s13054-016-1227-3
Prevalence and risk factors of hypotension associated with preload-dependence during intermittent hemodialysis in critically ill patients
Abstract
Background: Hypotension is a frequent complication of intermittent hemodialysis (IHD) performed in intensive care units (ICUs). Passive leg raising (PLR) combined with continuous measurement of cardiac output is highly reliable to identify preload dependence, and may provide new insights into the mechanisms involved in IHD-related hypotension. The aim of this study was to assess prevalence and risk factors of preload dependence-related hypotension during IHD in the ICU.
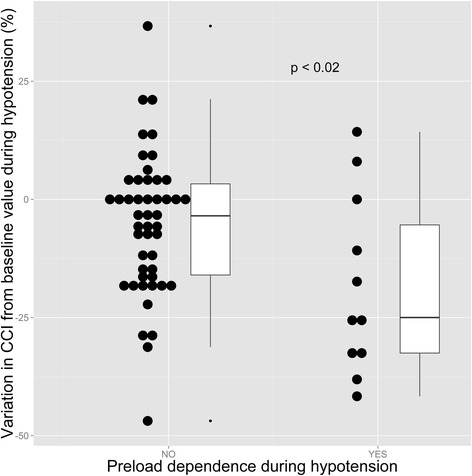
Methods: A single-center prospective observational study performed on ICU patients undergoing IHD for acute kidney injury and monitored with a PiCCO® device. Primary end points were the prevalence of hypotension (defined as a mean arterial pressure below 65 mm Hg) and hypotension associated with preload dependence. Preload dependence was assessed by the passive leg raising test, and considered present if the systolic ejection volume increased by at least 10% during the test, as assessed continuously by the PiCCO® device.
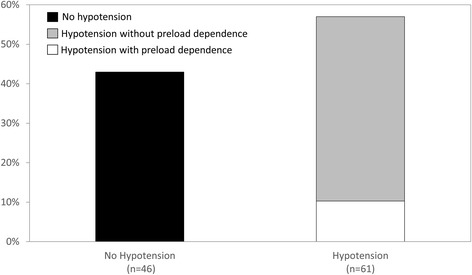
Results: Forty-seven patients totaling 107 IHD sessions were included. Hypotension was observed in 61 IHD sessions (57%, CI95%: 47-66%) and was independently associated with inotrope administration, higher SOFA score, lower time lag between ICU admission and IHD session, and lower MAP at IHD session onset. Hypotension associated with preload dependence was observed in 19% (CI95%: 10-31%) of sessions with hypotension, and was associated with mechanical ventilation, lower SAPS II, higher pulmonary vascular permeability index (PVPI) and dialysate sodium concentration at IHD session onset. ROC curve analysis identified PVPI and mechanical ventilation as the only variables with significant diagnostic performance to predict hypotension associated with preload dependence (respective AUC: 0.68 (CI95%: 0.53-0.83) and 0.69 (CI95%: 0.54-0.85). A PVPI ≥ 1.6 at IHD session onset predicted occurrence of hypotension associated with preload dependence during IHD with a sensitivity of 91% (CI95%: 59-100%), and a specificity of 53% (CI95%: 42-63%).
Conclusions: The majority of hypotensive episodes occurring during intermittent hemodialysis are unrelated to preload dependence and should not necessarily lead to reduction of fluid removal by hemodialysis. However, high PVPI at IHD session onset and mechanical ventilation are risk factors of preload dependence-related hypotension, and should prompt reduction of planned fluid removal during the session, and/or an increase in session duration.
Figures
Comment in
-
Renal Replacement Therapy: Timing of Initiation and Intradialytic Hypotension.Am J Respir Crit Care Med. 2017 Jul 1;196(1):102-104. doi: 10.1164/rccm.201611-2375RR. Am J Respir Crit Care Med. 2017. PMID: 28463519 No abstract available.
References
-
- Kidney Disease Improving Global Outcomes (KDIGO) Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012; 2:1–138.
-
- du Cheyron D, Terzi N, Seguin A, Valette X, Prevost F, Ramakers M, et al. Use of online blood volume and blood temperature monitoring during haemodialysis in critically ill patients with acute kidney injury: a single-centre randomized controlled trial. Nephrol Dial Transplant. 2013;28:430–7. doi: 10.1093/ndt/gfs124. - DOI - PubMed
-
- Vinsonneau C, Camus C, Combes A, Costa de Beauregard MA, Klouche K, Boulain T, et al. Continuous venovenous haemodiafiltration versus intermittent haemodialysis for acute renal failure in patients with multiple-organ dysfunction syndrome: a multicentre randomised trial. Lancet. 2006;368:379–85. doi: 10.1016/S0140-6736(06)69111-3. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
