

HCV kinetic and modeling analyses indicate similar time to cure among sofosbuvir combination regimens with daclatasvir, simeprevir or ledipasvir
- PMID: 26907973
- PMCID: PMC5081285
- DOI: 10.1016/j.jhep.2016.02.022
HCV kinetic and modeling analyses indicate similar time to cure among sofosbuvir combination regimens with daclatasvir, simeprevir or ledipasvir
Abstract
Background & aims: Recent clinical trials of direct-acting-antiviral agents (DAAs) against hepatitis C virus (HCV) achieved >90% sustained virological response (SVR) rates, suggesting that cure often took place before the end of treatment (EOT). We sought to evaluate retrospectively whether early response kinetics can provide the basis to individualize therapy to achieve optimal results while reducing duration and cost.
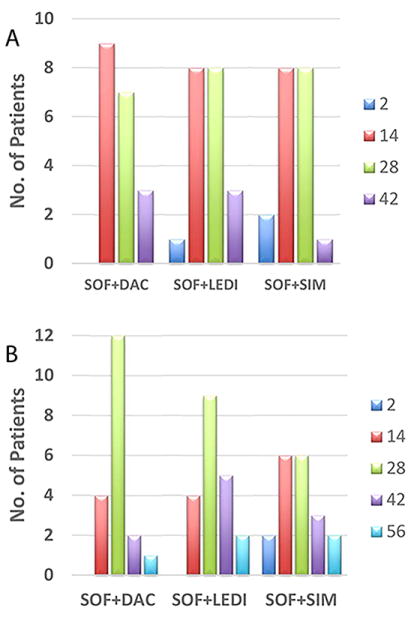
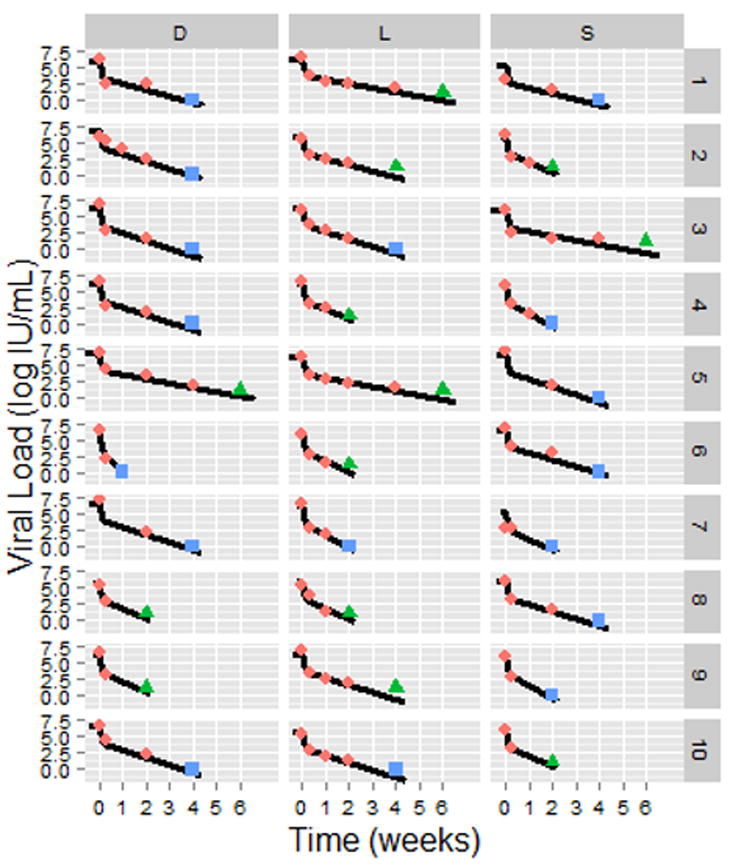
Methods: 58 chronic HCV patients were treated with 12-week sofosbuvir+simeprevir (n=19), sofosbuvir+daclatasvir (n=19), or sofosbuvir+ledipasvir in three French referral centers. HCV was measured at baseline, day 2, every other week, EOT and 12weeks post EOT. Mathematical modeling was used to predict the time to cure, i.e., <1 virus copy in the entire extracellular body fluid.
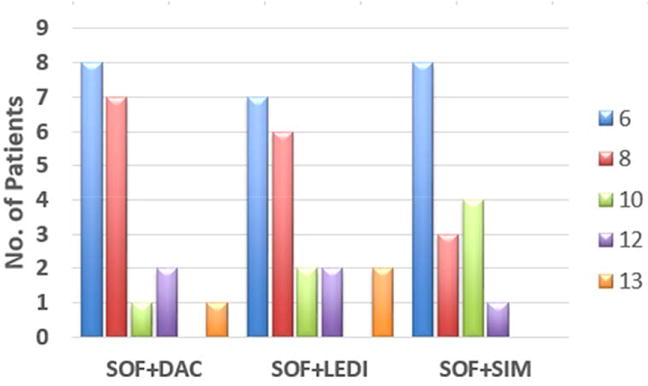
Results: All but one patient who relapsed achieved SVR. Mean age was 60±11years, 53% were male, 86% HCV genotype-1, 9% HIV coinfected, 43% advanced fibrosis (F3), and 57% had cirrhosis. At weeks 2, 4 and 6, 48%, 88% and 100% of patients had HCV<15IU/ml, with 27%, 74% and 91% of observations having target not detected, respectively. Modeling results predicted that 23 (43%), 16 (30%), 7 (13%), 5 (9%) and 3 (5%) subjects were predicted to reach cure within 6, 8, 10, 12 and 13weeks of therapy, respectively. The modeling suggested that the patient who relapsed would have benefitted from an additional week of sofosbuvir+ledipasvir. Adjusting duration of treatment according to the modeling predicts reduced medication costs of 43-45% and 17-30% in subjects who had HCV<15IU/ml at weeks 2 and 4, respectively.
Conclusions: The use of early viral kinetic analysis has the potential to individualize duration of DAA therapy with a projected average cost saving of 16-20% per 100-treated persons.
Keywords: Duration of therapy; HCV; Mathematical modeling; SVR; Viral kinetics.
Copyright © 2016 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Disclosures: None of the authors has any financial interest or conflict of interest related to this research. Writing Assistance: None.
Figures
References
-
- Bourliere M, Bronowicki JP, de Ledinghen V, Hezode C, Zoulim F, Mathurin P, et al. Lancet Infect Dis. 2015;15:397–404. - PubMed
-
- Reddy KR, Bourliere M, Sulkowski M, Omata M, Zeuzem S, Feld JJ, et al. Hepatology. 2015
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
