

Identifying determinants of heterogeneous transmission dynamics of the Middle East respiratory syndrome (MERS) outbreak in the Republic of Korea, 2015: a retrospective epidemiological analysis
- PMID: 26908522
- PMCID: PMC4769415
- DOI: 10.1136/bmjopen-2015-009936
Identifying determinants of heterogeneous transmission dynamics of the Middle East respiratory syndrome (MERS) outbreak in the Republic of Korea, 2015: a retrospective epidemiological analysis
Abstract
Objectives: To investigate the heterogeneous transmission patterns of Middle East respiratory syndrome (MERS) in the Republic of Korea, with a particular focus on epidemiological characteristics of superspreaders.
Design: Retrospective epidemiological analysis.
Setting: Multiple healthcare facilities of secondary and tertiary care centres in an urban setting.
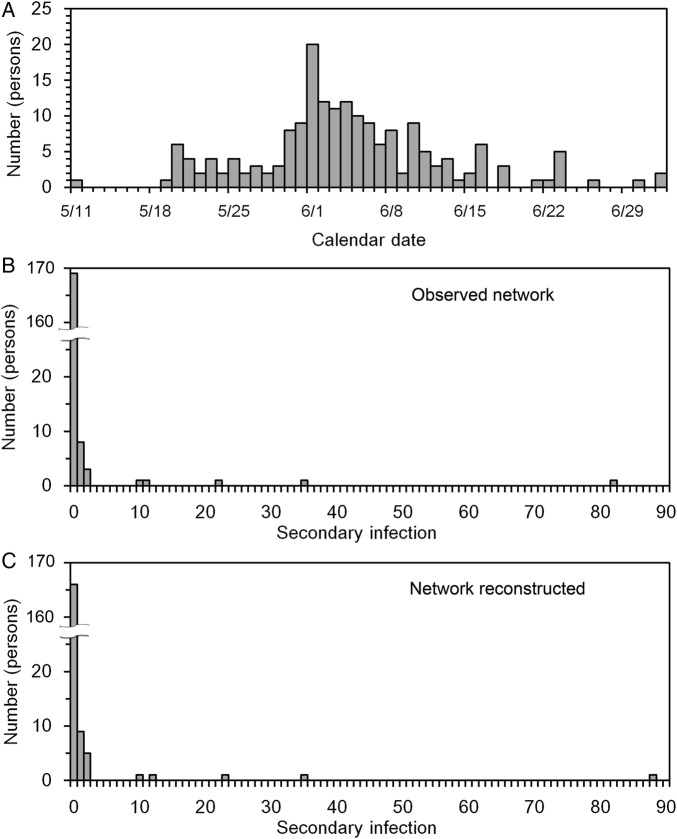
Participants: A total of 185 laboratory-confirmed cases with partially known dates of illness onset and most likely sources of infection.
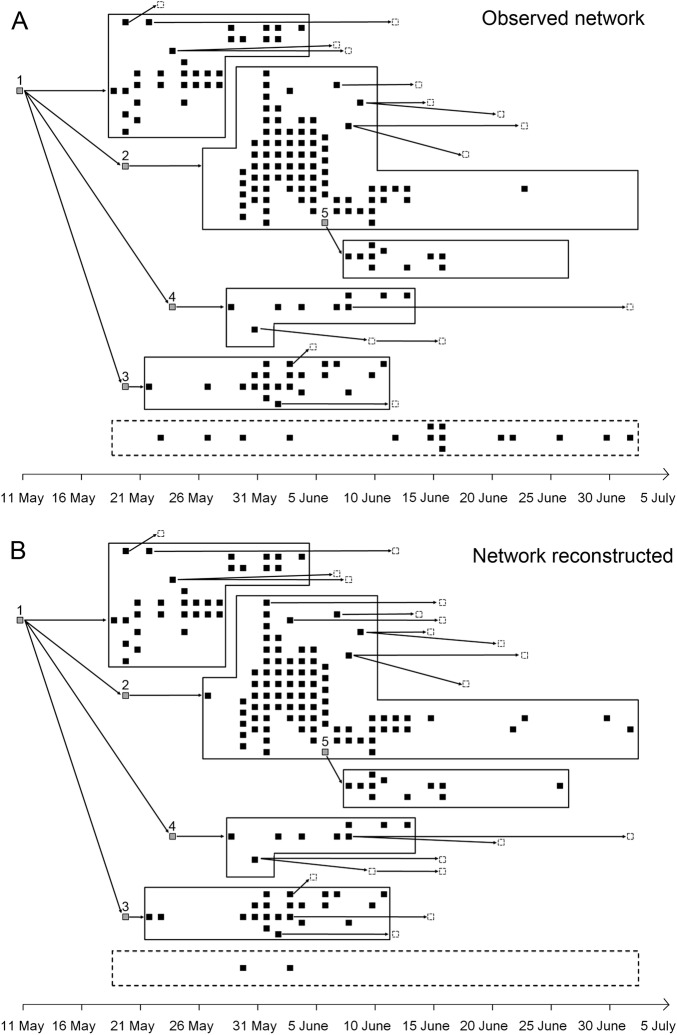
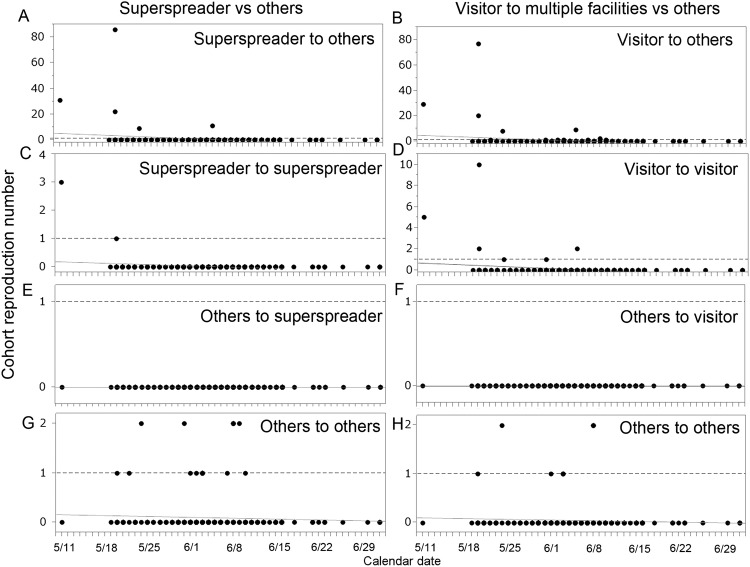
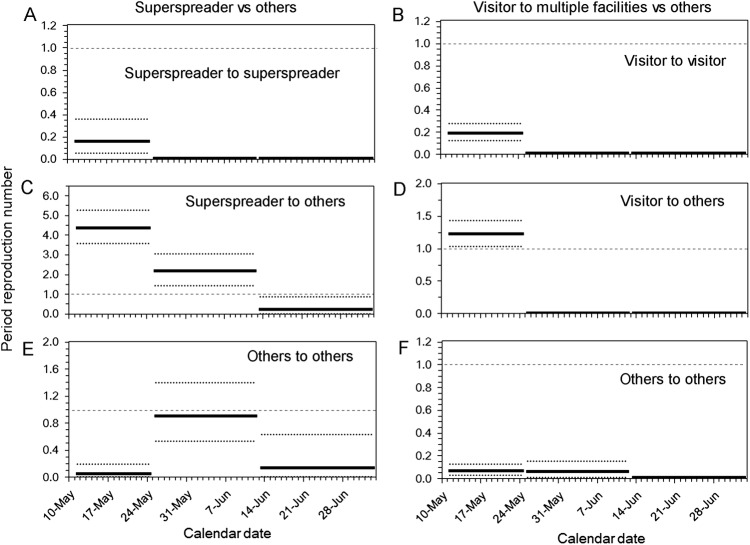
Primary and secondary outcome measures: Superspreaders were identified using the transmission tree. The reproduction number, that is, the average number of secondary cases produced by a single primary case, was estimated as a function of time and according to different types of hosts.
Results: A total of five superspreaders were identified. The reproduction number throughout the course of the outbreak was estimated at 1.0 due to reconstruction of the transmission tree, while the variance of secondary cases generated by a primary case was 52.1. All of the superspreaders involved in this outbreak appeared to have generated a substantial number of contacts in multiple healthcare facilities (association: p<0.01), generating on average 4.0 (0.0-8.6) and 28.6 (0.0-63.9) secondary cases among patients who visited multiple healthcare facilities and others. The time-dependent reproduction numbers declined substantially below the value of 1 on and after 13 June 2015.
Conclusions: Superspreaders who visited multiple facilities drove the epidemic by generating a disproportionate number of secondary cases. Our findings underscore the need to limit the contacts in healthcare settings. Contact tracing efforts could assist early laboratory testing and diagnosis of suspected cases.
Keywords: EPIDEMIOLOGY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources