

Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysis
- PMID: 26908524
- PMCID: PMC4769405
- DOI: 10.1136/bmjopen-2015-010003
Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysis
Abstract
Objectives: Pharmacists play a role in providing medication reconciliation. However, data on effectiveness on patients' clinical outcomes appear inconclusive. Thus, the aim of this study was to systematically investigate the effect of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions.
Design: Systematic review and meta-analysis.
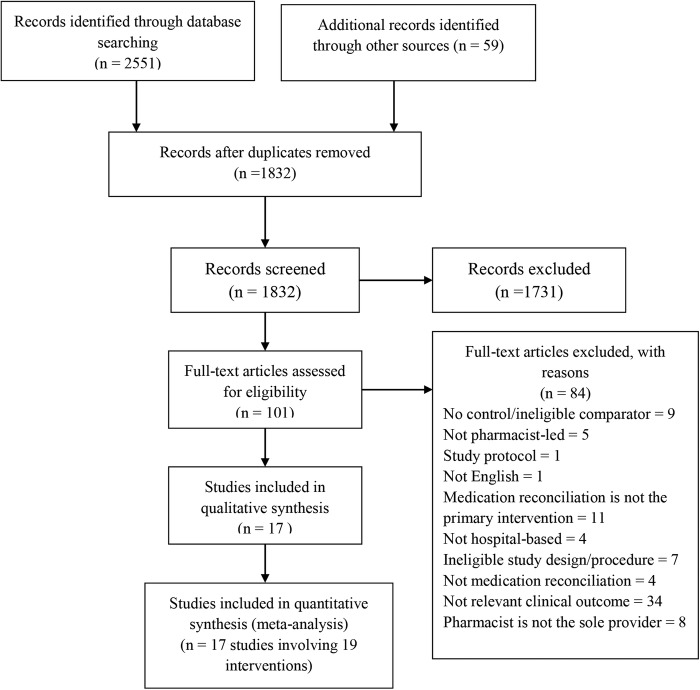
Methods: We searched PubMed, MEDLINE, EMBASE, IPA, CINHAL and PsycINFO from inception to December 2014. Included studies were all published studies in English that compared the effectiveness of pharmacist-led medication reconciliation interventions to usual care, aimed at improving medication reconciliation programmes. Meta-analysis was carried out using a random effects model, and subgroup analysis was conducted to determine the sources of heterogeneity.
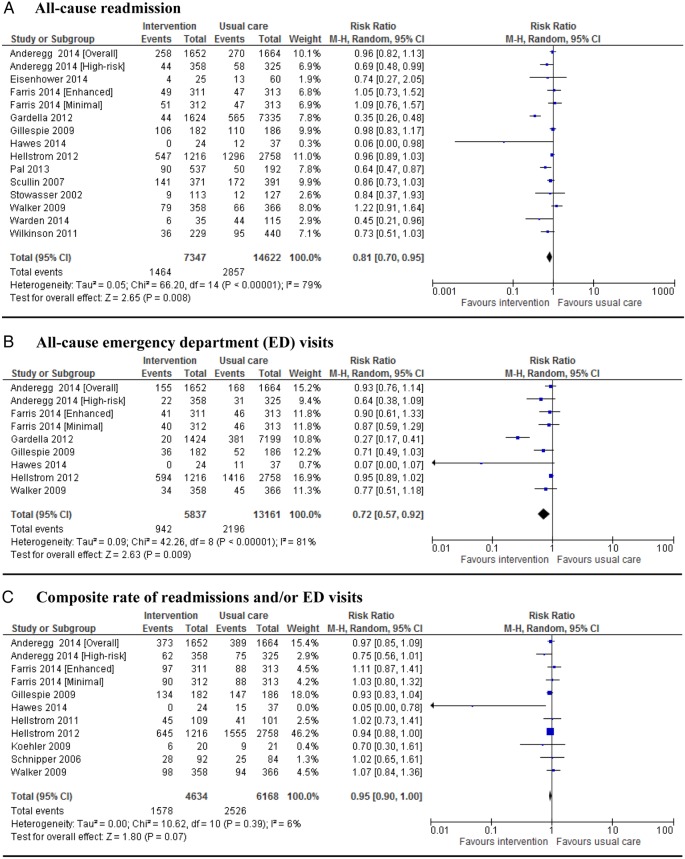
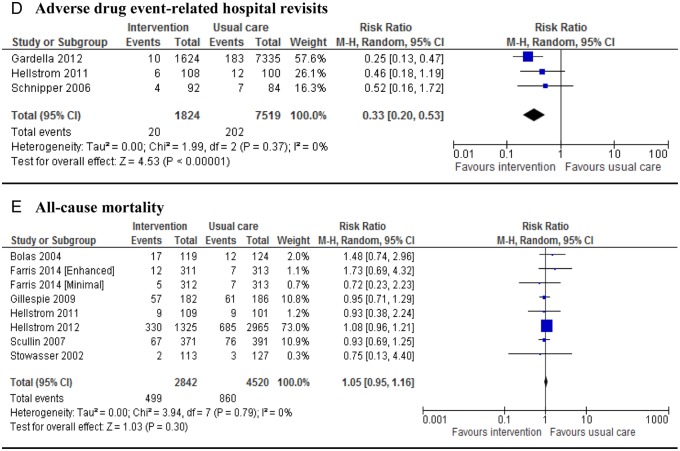
Results: 17 studies involving 21,342 adult patients were included. Eight studies were randomised controlled trials (RCTs). Most studies targeted multiple transitions and compared comprehensive medication reconciliation programmes including telephone follow-up/home visit, patient counselling or both, during the first 30 days of follow-up. The pooled relative risks showed a more substantial reduction of 67%, 28% and 19% in adverse drug event-related hospital revisits (RR 0.33; 95% CI 0.20 to 0.53), emergency department (ED) visits (RR 0.72; 95% CI 0.57 to 0.92) and hospital readmissions (RR 0.81; 95% CI 0.70 to 0.95) in the intervention group than in the usual care group, respectively. The pooled data on mortality (RR 1.05; 95% CI 0.95 to 1.16) and composite readmission and/or ED visit (RR 0.95; 95% CI 0.90 to 1.00) did not differ among the groups. There was significant heterogeneity in the results related to readmissions and ED visits, however. Subgroup analyses based on study design and outcome timing did not show statistically significant results.
Conclusion: Pharmacist-led medication reconciliation programmes are effective at improving post-hospital healthcare utilisation. This review supports the implementation of pharmacist-led medication reconciliation programmes that include some component aimed at improving medication safety.
Keywords: Medication reconciliation; medication discrepancies; medication errors; medication review; pharmacists.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- Institute for Healthcare Improvement. Medication reconciliation review. http://www.ihi.org/resources/Pages/Tools/MedicationReconciliationReview.... (accessed 30 Dec 2014).
-
- Rozich JD, Howard RJ, Justeson JM et al. Standardization as a mechanism to improve safety in health care. Jt Comm J Qual Saf 2004;30:5–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical