

Cross-sectional study of the prehospital management of adult patients with a suspected seizure (EPIC1)
- PMID: 26908532
- PMCID: PMC4769426
- DOI: 10.1136/bmjopen-2015-010573
Cross-sectional study of the prehospital management of adult patients with a suspected seizure (EPIC1)
Abstract
Objectives: Suspected seizures are a common reason for emergency calls to ambulance services. Prehospital management of these patients is an important element of good quality care. The aim of this study, conducted in a regional ambulance service in the UK, was to quantify the number of emergency telephone calls for suspected seizures in adults, the associated costs, and to describe the patients' characteristics, their prehospital management and their immediate outcomes.
Design: Quantitative cross-sectional study using routinely collected data and a detailed review of the clinical records of a consecutive series of adult patients (≥ 16 years).
Setting: A regional ambulance service within the National Health Service in England.
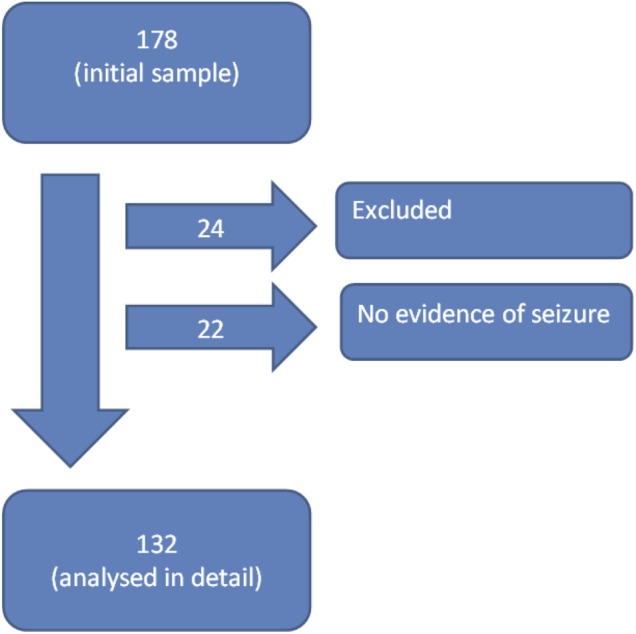
Participants: Cross-sectional data from all 605,481 adult emergency incidents managed by the ambulance service from 1 April 2012 to 31 March 2013. We selected a consecutive series of 178 individual incidents from May 2012 for more detailed analysis (132 after exclusions and removal of non-seizure cases).
Results: Suspected seizures made up 3.3% of all emergency incidents. True medical emergencies were uncommon but 3.3% had partially occluded airways, 6.8% had ongoing seizure activity and 59.1% had clinical problems in addition to the seizure (29.1% involving injury). Emergency vehicles were dispatched for 97.2% of suspected seizures, the seizure had terminated on arrival in 93.2% of incidents, 75% of these patients were transported to hospital. The estimated emergency management cost per annum of suspected seizures in the English ambulance services is £45.2 million (€64.0 million, $68.6 million).
Conclusions: Many patients with suspected seizures could potentially be treated more effectively and at lower cost by modifying ambulance call handling protocols. The development of innovative care pathways could give call handlers and paramedics alternatives to hospital transportation. Increased adoption of care plans could reduce 999 calls and could increase the rates of successful home or community treatment.
Keywords: ACCIDENT & EMERGENCY MEDICINE; HEALTH SERVICES ADMINISTRATION & MANAGEMENT; NEUROLOGY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- Malmgren K, Reuber M, Appleton R. Differential diagnosis of epilepsy. Oxford Textbook of Epilepsy and Epileptic Seizures Oxford University Press, 2013.
-
- Joint Royal Colleges Ambulance Liaison Committee. UK Ambulance Services Clinical Practice Guidelines 2013. Bristol: Class Professional Publishing, 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous