

Field Synopsis of Sex in Clinical Prediction Models for Cardiovascular Disease
- PMID: 26908865
- PMCID: PMC5573163
- DOI: 10.1161/CIRCOUTCOMES.115.002473
Field Synopsis of Sex in Clinical Prediction Models for Cardiovascular Disease
Abstract
Background: Several widely used risk scores for cardiovascular disease (CVD) incorporate sex effects, yet there has been no systematic summary of the role of sex in clinical prediction models (CPMs). To better understand the potential of these models to support sex-specific care, we conducted a field synopsis of sex effects in CPMs for CVD.
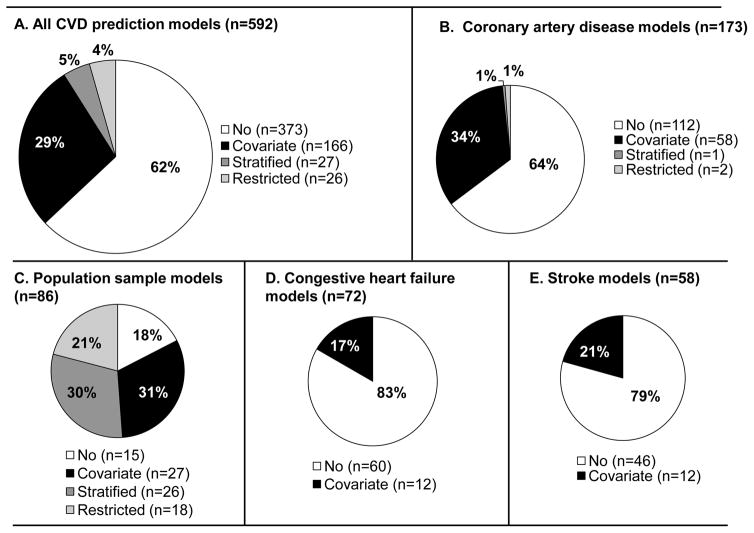
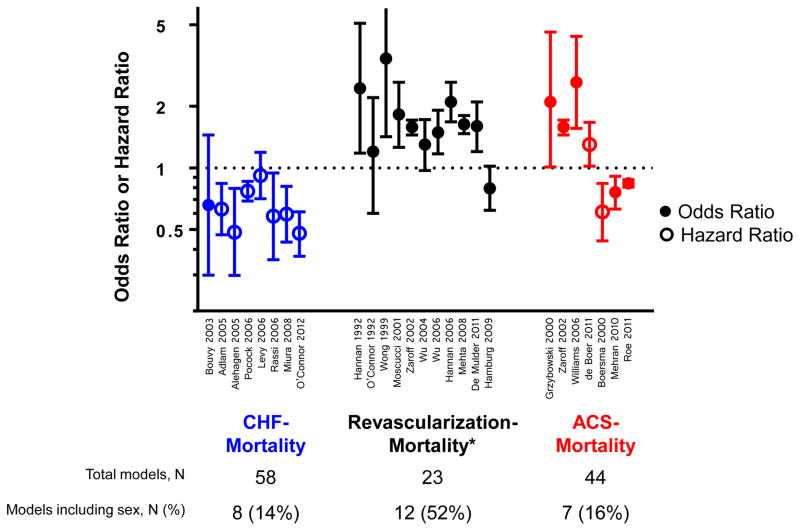
Methods and results: We identified CPMs in the Tufts Predictive Analytics and Comparative Effectiveness CPM Registry, a comprehensive database of CVD CPMs published from January 1990 to May 2012. We report the proportion of models including sex effects on CVD incidence or prognosis, summarize the directionality of the predictive effects of sex, and explore factors influencing the inclusion of sex. Of 592 CVD-related CPMs, 193 (33%) included sex as a predictor or presented sex-stratified models. Sex effects were included in 78% (53/68) of models predicting incidence of CVD in a general population, versus only 35% (59/171), 21% (12/58), and 17% (12/72) of models predicting outcomes in patients with coronary artery disease, stroke, and heart failure, respectively. Among sex-including CPMs, women with heart failure were at lower mortality risk in 8 of 8 models; women undergoing revascularization for coronary artery disease were at higher mortality risk in 10 of 12 models. Factors associated with the inclusion of sex effects included the number of outcome events and using cohorts at-risk for CVD (rather than with established CVD).
Conclusions: Although CPMs hold promise for supporting sex-specific decision making in CVD clinical care, sex effects are included in only one third of published CPMs.
Keywords: cardiovascular diseases; prevention and control; prognosis; risk factors; sex; sex characteristics; women.
© 2016 American Heart Association, Inc.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
