

Orthostatic Cerebral Hypoperfusion Syndrome
- PMID: 26909037
- PMCID: PMC4754393
- DOI: 10.3389/fnagi.2016.00022
Orthostatic Cerebral Hypoperfusion Syndrome
Abstract
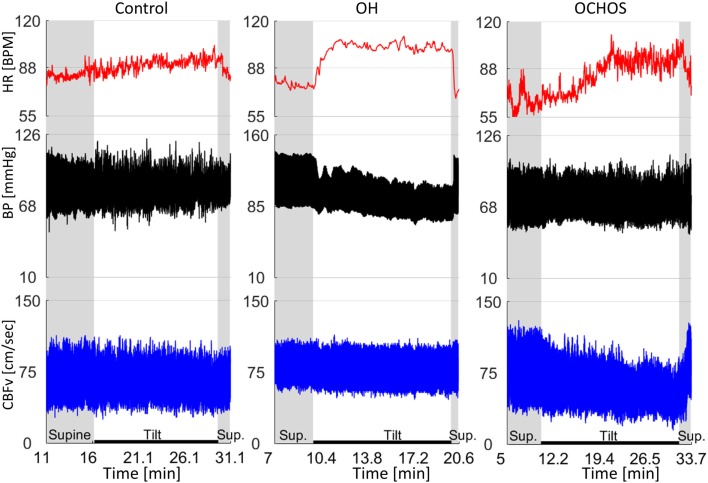
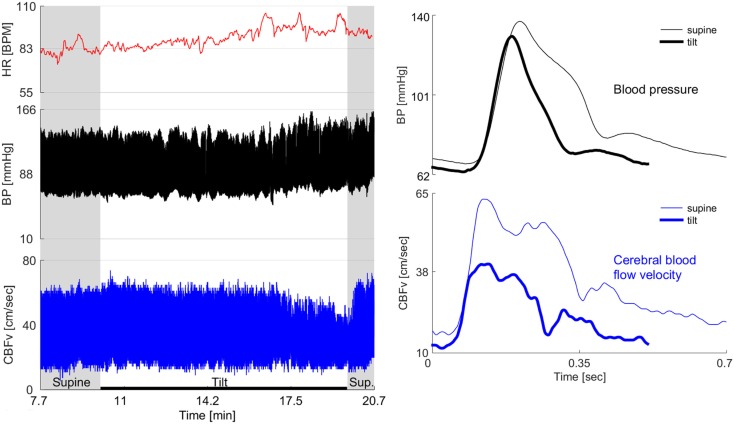
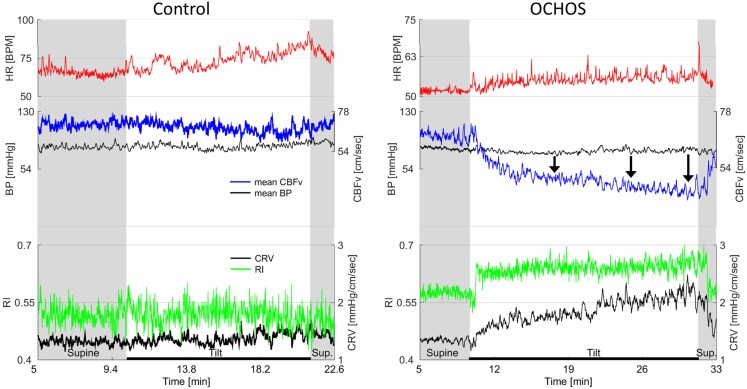
Objective: Orthostatic dizziness without orthostatic hypotension is common but underlying pathophysiology is poorly understood. This study describes orthostatic cerebral hypoperfusion syndrome (OCHOs). OCHOs is defined by (1) abnormal orthostatic drop of cerebral blood flow velocity (CBFv) during the tilt test and (2) absence of orthostatic hypotension, arrhythmia, vascular abnormalities, or other causes of abnormal orthostatic CBFv.
Methods: This retrospective study included patients referred for evaluation of unexplained orthostatic dizziness. Patients underwent standardized autonomic testing, including 10 min of tilt test. The following signals were monitored: heart rate, end tidal CO2, blood pressure, and CBFv from the middle cerebral artery using transcranial Doppler. Patients were screened for OCHOs. Patients who fulfilled the OCHOs criteria were compared to age- and gender-matched controls.
Results: From 1279 screened patients, 102 patients (60/42 women/men, age 51.1 ± 14.9, range 19-84 years) fulfilled criteria of OCHOs. There was no difference in baseline supine hemodynamic variables between OCHOs and the control group. During the tilt, mean CBFv decreased 24.1 ± 8.2% in OCHOs versus 4.2 ± 5.6% in controls (p < 0.0001) without orthostatic hypotension in both groups. Supine mean blood pressure (OCHOs/controls, 90.5 ± 10.6/91.1 ± 9.4 mmHg, p = 0.62) remained unchanged during the tilt (90.4 ± 9.7/92.1 ± 9.6 mmHg, p = 0.2). End tidal CO2 and heart rate responses to the tilt were normal and equal in both groups.
Conclusion: OCHOs is a novel syndrome of low orthostatic CBFv. Two main pathophysiological mechanisms are proposed, including active cerebral vasoconstriction and passive increase of peripheral venous compliance. OCHOs may be a common cause of orthostatic dizziness.
Keywords: OCHOs; OH; POTS; QASAT; hypoperfusion; hypotension; orthostatic.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources