

Mycoplasma pneumoniae Epidemiology in England and Wales: A National Perspective
- PMID: 26909073
- PMCID: PMC4754400
- DOI: 10.3389/fmicb.2016.00157
Mycoplasma pneumoniae Epidemiology in England and Wales: A National Perspective
Abstract
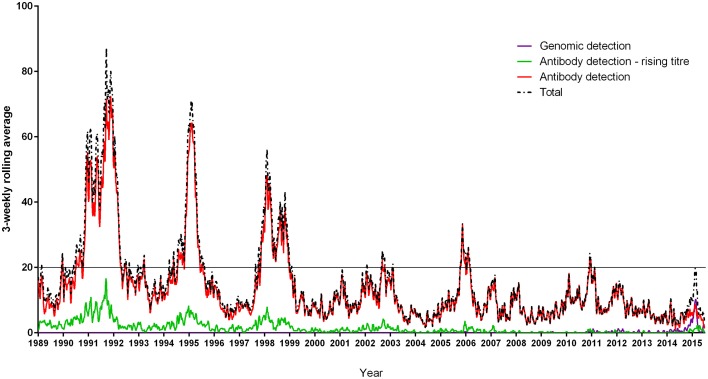
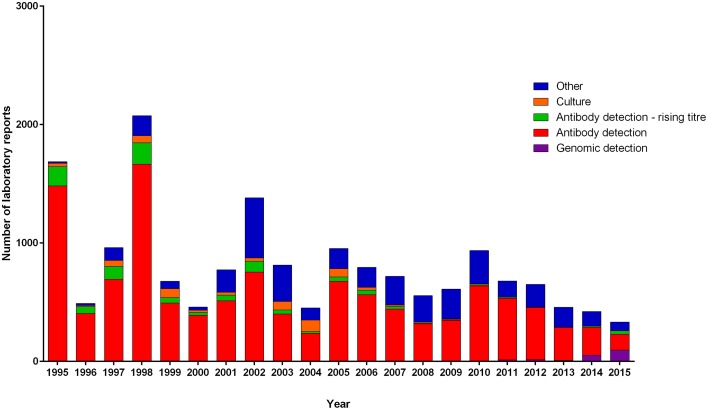
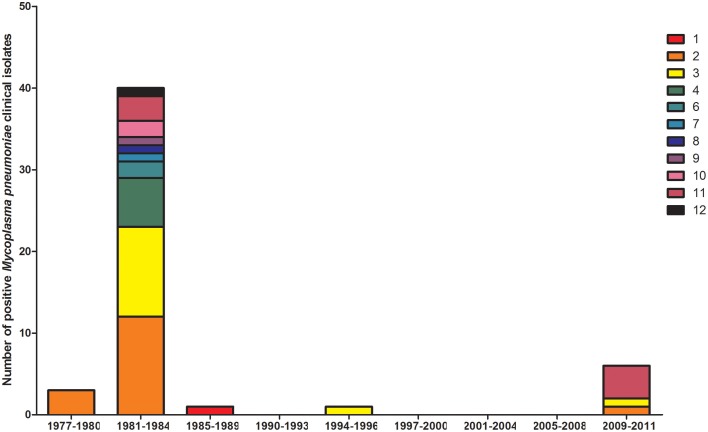
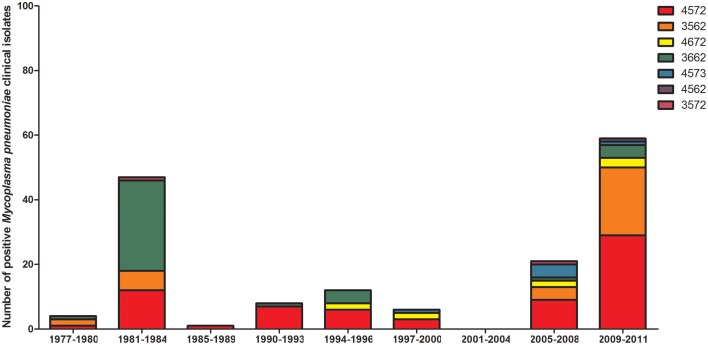
Investigations of patients with suspected Mycoplasma pneumoniae infection have been undertaken in England since the early 1970s. M. pneumoniae is a respiratory pathogen that is a common cause of pneumonia and may cause serious sequelae such as encephalitis and has been documented in children with persistent cough. The pathogen is found in all age groups, with higher prevalence in children aged 5-14 years. In England, recurrent epidemic periods have occurred at ~4-yearly intervals. In addition, low-level sporadic infection occurs with seasonal peaks from December to February. Voluntarily reports from regional laboratories and hospitals in England from 1975 to 2015 were collated by Public Health England for epidemiological analysis. Further data pertaining cases of note and specimens submitted to Public Health England from 2005 to 2015 for confirmation, molecular typing is included.
Keywords: England; Mycoplasma pneumoniae; epidemiology; microbiology; wales.
Figures
References
-
- Bebear C., Robertson J. A. (1996). Determination of minimal inhibitory concentration, in Molecular and Diagnostic Procedures in Mycoplasmology, eds Tully J. G., Razin S. (New York, NY: Academic Press; ), 189–197.
LinkOut - more resources
Full Text Sources
Other Literature Sources