

Outcomes of Cardiopulmonary Resuscitation and Estimation of Healthcare Costs in Potential 'Do Not Resuscitate' Cases
- PMID: 26909209
- PMCID: PMC4746039
- DOI: 10.18295/squmj.2016.16.01.006
Outcomes of Cardiopulmonary Resuscitation and Estimation of Healthcare Costs in Potential 'Do Not Resuscitate' Cases
Abstract
Objectives: Cardiopulmonary resuscitation (CPR) is a life-saving procedure which may fail if applied unselectively. 'Do not resuscitate' (DNR) policies can help avoid futile life-saving attempts among terminally-ill patients. This study aimed to assess CPR outcomes and estimate healthcare costs in potential DNR cases.
Methods: This retrospective study was carried out between March and June 2014 and included 50 adult cardiac arrest patients who had undergone CPR at Sultan Qaboos Hospital in Salalah, Oman. Medical records were reviewed and treating teams were consulted to determine DNR eligibility. The outcomes, clinical risk categories and associated healthcare costs of the DNR candidates were assessed.
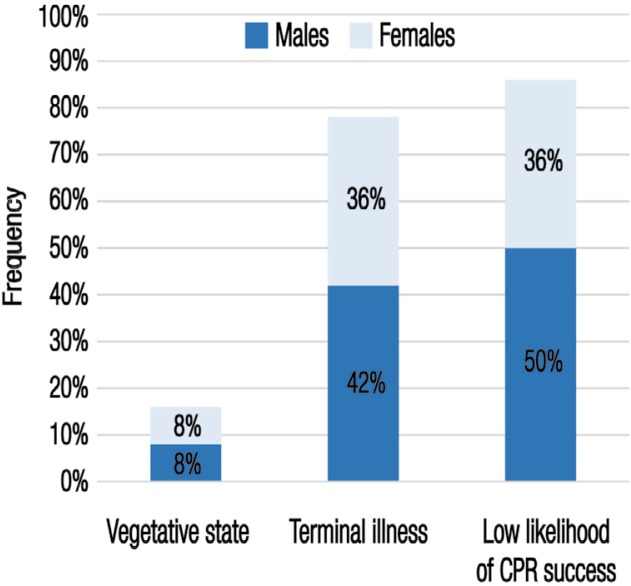
Results: Two-thirds of the potential DNR candidates were ≥60 years old. Eight patients (16%) were in a vegetative state, 39 (78%) had an irreversible terminal illness and 43 (86%) had a low likelihood of successful CPR. Most patients (72%) met multiple criteria for DNR eligibility. According to clinical risk categories, these patients had terminal malignancies (30%), recent massive strokes (16%), end-stage organ failure (30%) or were bed-bound (50%). Initial CPR was unsuccessful in 30 patients (60%); the remaining 20 patients (40%) were initially resuscitated but subsequently died, with 70% dying within 24 hours. These patients were ventilated for an average of 5.6 days, with four patients (20%) requiring >15 days of ventilation. The average healthcare cost per patient was USD $1,958.9.
Conclusion: With careful assessment, potential DNR patients can be identified and futile CPR efforts avoided. Institutional DNR policies may help to reduce healthcare costs and improve services.
Keywords: Cardiopulmonary Resuscitation; Do Not Resuscitate Orders; Healthcare Costs; Medical Futility; Oman; Persistent Vegetative State; Terminally Ill.
Figures
Similar articles
-
Association of medical futility with do-not-resuscitate (DNR) code status in hospitalised patients.J Med Ethics. 2021 Jan 29:medethics-2020-106977. doi: 10.1136/medethics-2020-106977. Online ahead of print. J Med Ethics. 2021. PMID: 33514639
-
A descriptive analysis of obstacles to fulfilling the end of life care goals among cardiac arrest patients.Resusc Plus. 2021 Aug 27;8:100160. doi: 10.1016/j.resplu.2021.100160. eCollection 2021 Dec. Resusc Plus. 2021. PMID: 34485954 Free PMC article.
-
The implications of dying cancer patients' talk on cardiopulmonary resuscitation and do-not-resuscitate orders.Qual Health Res. 2007 Apr;17(4):442-55. doi: 10.1177/1049732307299198. Qual Health Res. 2007. PMID: 17416698
-
[Cardiopulmonary resuscitation and do not resuscitate orders].Rev Med Chil. 2007 May;135(5):669-79. Epub 2007 Jul 9. Rev Med Chil. 2007. PMID: 17657338 Review. Spanish.
-
Cardiopulmonary resuscitation: are practitioners being realistic?Br J Nurs. 1999 Jun 24-Jul 7;8(12):810-4. doi: 10.12968/bjon.1999.8.12.6577. Br J Nurs. 1999. PMID: 10670299 Review.
Cited by
-
Predictive Factors for Cardiopulmonary Resuscitation Failure.Indian J Palliat Care. 2021 Jul-Sep;27(3):426-430. doi: 10.25259/IJPC_447_20. Epub 2021 Nov 9. Indian J Palliat Care. 2021. PMID: 34898936 Free PMC article.
-
Pediatricians' Perceptions Toward Do Not Resuscitate: A Survey in Saudi Arabia and Literature Review.Adv Med Educ Pract. 2020 Jan 6;11:1-8. doi: 10.2147/AMEP.S228399. eCollection 2020. Adv Med Educ Pract. 2020. PMID: 32021536 Free PMC article.
-
Choosing and Doing wisely: triage level I resuscitation a possible new field for starting palliative care and avoiding low-value care - a nationwide matched-pair retrospective cohort study in Taiwan.BMC Palliat Care. 2020 Jun 20;19(1):87. doi: 10.1186/s12904-020-00590-5. BMC Palliat Care. 2020. PMID: 32563245 Free PMC article.
-
The do-not-resuscitate order for terminal cancer patients in mainland China: A retrospective study.Medicine (Baltimore). 2018 May;97(18):e0588. doi: 10.1097/MD.0000000000010588. Medicine (Baltimore). 2018. PMID: 29718859 Free PMC article.
-
Death and do-not-resuscitate order in the emergency department: A single-center three-year retrospective study in the Chinese mainland.World J Emerg Med. 2020;11(4):231-237. doi: 10.5847/wjem.j.1920-8642.2020.04.005. World J Emerg Med. 2020. PMID: 33014219 Free PMC article.
References
-
- Tossach WA. A man dead in appearance recovered by distending the lungs with air. Med Essays Obs. 1744;5:605–8.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous