

Magnetic resonance imaging of intraoral hard and soft tissues using an intraoral coil and FLASH sequences
- PMID: 26910905
- PMCID: PMC5101280
- DOI: 10.1007/s00330-016-4254-1
Magnetic resonance imaging of intraoral hard and soft tissues using an intraoral coil and FLASH sequences
Abstract
Objectives: To ascertain the feasibility of MRI as a non-ionizing protocol for routine dentomaxillofacial diagnostic imaging. Wireless coils were used for MRI of intraoral hard and soft tissues.
Methods: FLASH MRI was applied in vivo with a mandible voxel size of 250 × 250 × 500 μm3, FOV of 64 × 64 × 28 mm3 and acquisition time of 3:57 min and with a maxilla voxel size of 350 μm3 and FOV of 34 cm3 in 6:40 min. Ex vivo imaging was performed in 4:38 min, with a resolution of 200 μm3 and FOV of 36.5 cm3. Cone beam (CB) CT of the mandible and subjects were acquired. MRI was compared to CBCT and histological sections. Deviations were calculated with intraclass correlation coefficient (ICC) and coefficient of variation (cv).
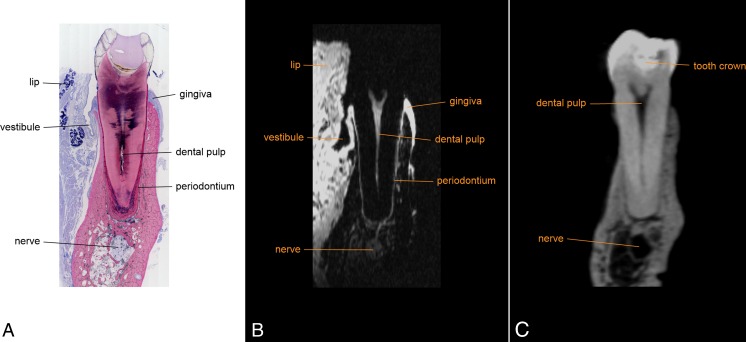
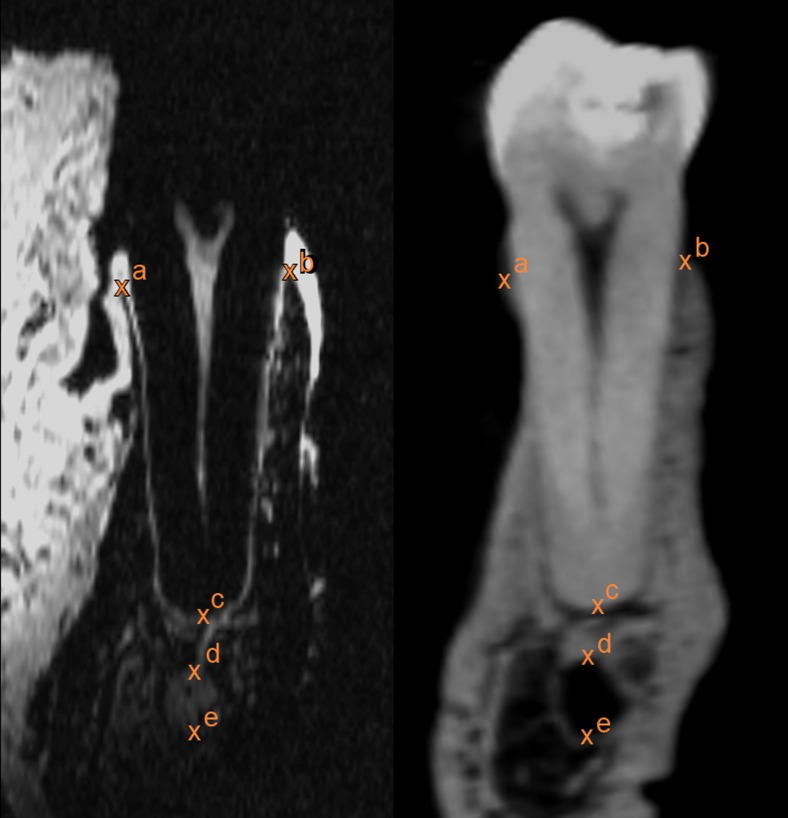
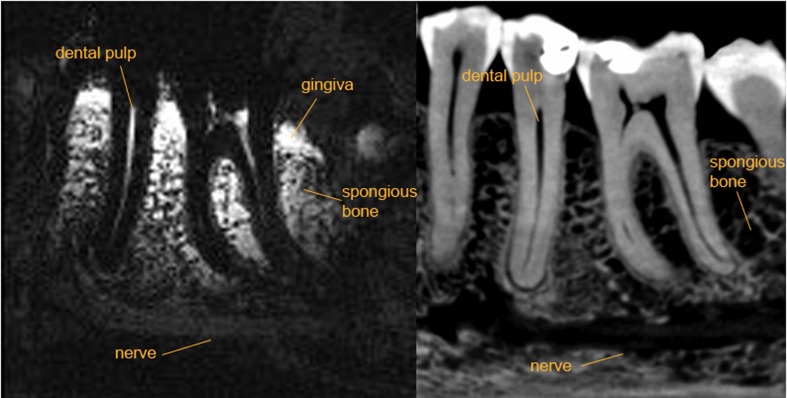
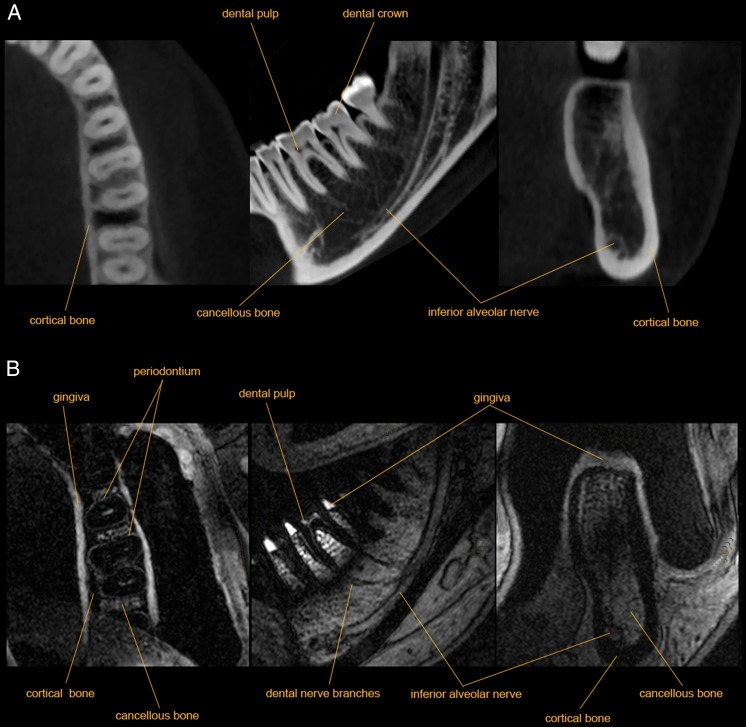
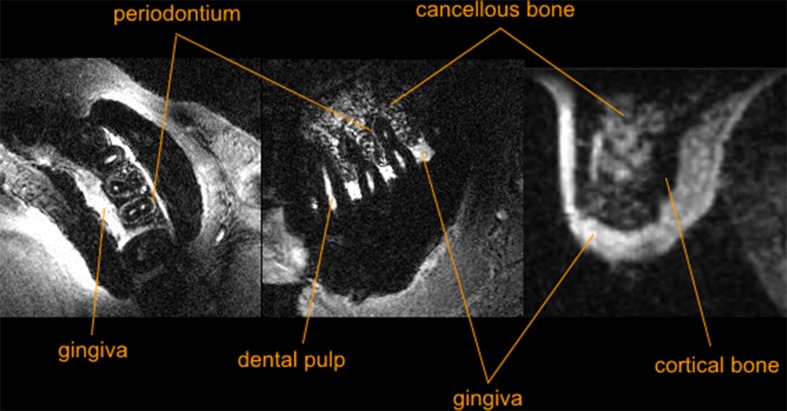
Results: A high congruence between CBCT, MRI and specimens was demonstrated. Hard and soft tissues including dental pulp, periodontium, gingiva, cancellous bone and mandibular canal contents were adequately displayed with MRI.
Conclusions: Imaging of select intraoral tissues was achieved using custom MRI protocols with an easily applicable intraoral coil in a clinically acceptable acquisition time. Comparison with CBCT and histological sections helped demonstrate dimensional accuracy of the MR images. The course of the mandibular canal was accurately displayed with CBCT and MRI.
Key points: • MRI is a clinically available diagnostic tool in dentistry • Intraoral hard and soft tissues can be imaged with a high resolution with MRI • The dimensional accuracy of MRI is comparable to cone beam CT.
Keywords: Accuracy; Cone beam computed tomography; Dental Implantation; Dimensional measurement; Magnetic resonance imaging.
Figures
Similar articles
-
Dental MRI using wireless intraoral coils.Sci Rep. 2016 Mar 29;6:23301. doi: 10.1038/srep23301. Sci Rep. 2016. PMID: 27021387 Free PMC article.
-
Geometric accuracy of magnetic resonance imaging-derived virtual 3-dimensional bone surface models of the mandible in comparison to computed tomography and cone beam computed tomography: A porcine cadaver study.Clin Implant Dent Relat Res. 2021 Oct;23(5):779-788. doi: 10.1111/cid.13033. Epub 2021 Jul 27. Clin Implant Dent Relat Res. 2021. PMID: 34318580
-
High-Resolution Single Tooth MRI With an Inductively Coupled Intraoral Coil-Can MRI Compete With CBCT?Invest Radiol. 2022 Nov 1;57(11):720-727. doi: 10.1097/RLI.0000000000000890. Epub 2022 May 25. Invest Radiol. 2022. PMID: 35640007
-
MRI for Dental Applications.Dent Clin North Am. 2018 Jul;62(3):467-480. doi: 10.1016/j.cden.2018.03.006. Dent Clin North Am. 2018. PMID: 29903562 Review.
-
[Cone Beam computerized tomography and implants].Rev Stomatol Chir Maxillofac. 2012 Sep;113(4):245-58. doi: 10.1016/j.stomax.2012.05.009. Epub 2012 Aug 11. Rev Stomatol Chir Maxillofac. 2012. PMID: 22889565 Review. French.
Cited by
-
Cone Beam Computed Tomography Panoramic Mandibular Indices in the Screening of Postmenopausal Women with Low Bone Mass: Correlations with Bone Quantity and Quality.Dent J (Basel). 2024 Aug 14;12(8):256. doi: 10.3390/dj12080256. Dent J (Basel). 2024. PMID: 39195100 Free PMC article.
-
In vivo comparison of MRI- and CBCT-based 3D cephalometric analysis: beginning of a non-ionizing diagnostic era in craniomaxillofacial imaging?Eur Radiol. 2020 Mar;30(3):1488-1497. doi: 10.1007/s00330-019-06540-x. Epub 2019 Dec 4. Eur Radiol. 2020. PMID: 31802215
-
Can lithium disilicate ceramic crowns be fabricated on the basis of CBCT data?Clin Oral Investig. 2019 Oct;23(10):3739-3748. doi: 10.1007/s00784-019-02802-6. Epub 2019 Feb 6. Clin Oral Investig. 2019. PMID: 30725188
-
Reliability and accuracy of dental MRI for measuring root canal length of incisors and canines: a clinical pilot study.Sci Rep. 2022 Aug 18;12(1):14068. doi: 10.1038/s41598-022-17889-3. Sci Rep. 2022. PMID: 35982139 Free PMC article.
-
MRI for the display of autologous onlay bone grafts during early healing-an experimental study.Dentomaxillofac Radiol. 2021 Feb 1;50(2):20200068. doi: 10.1259/dmfr.20200068. Epub 2020 Nov 17. Dentomaxillofac Radiol. 2021. PMID: 33201739 Free PMC article.
References
-
- National Council on Radiation Protection and Measurements (2009) Ionizing radiation exposure of the population of the United States. Bethesda, Md: National Council on Radiation Protection and Measurements
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
