

Magnetic resonance analysis of malignant transformation in recurrent glioma
- PMID: 26911151
- PMCID: PMC4933480
- DOI: 10.1093/neuonc/now008
Magnetic resonance analysis of malignant transformation in recurrent glioma
Abstract
Background: Patients with low-grade glioma (LGG) have a relatively long survival, and a balance is often struck between treating the tumor and impacting quality of life. While lesions may remain stable for many years, they may also undergo malignant transformation (MT) at the time of recurrence and require more aggressive intervention. Here we report on a state-of-the-art multiparametric MRI study of patients with recurrent LGG.
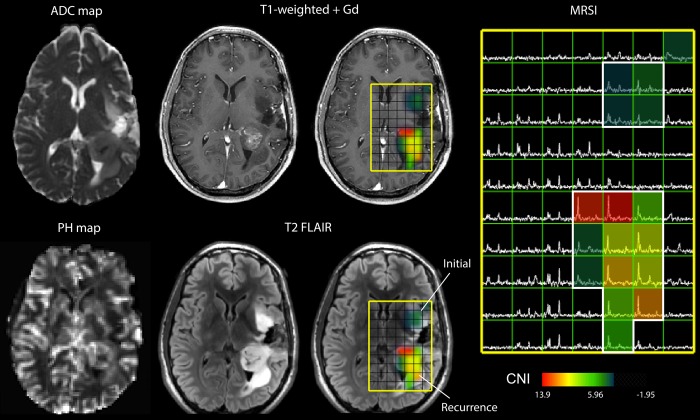
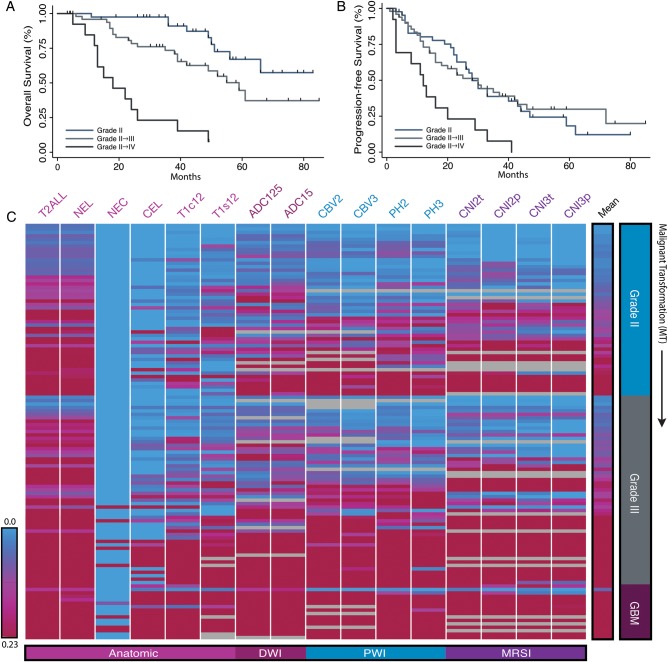
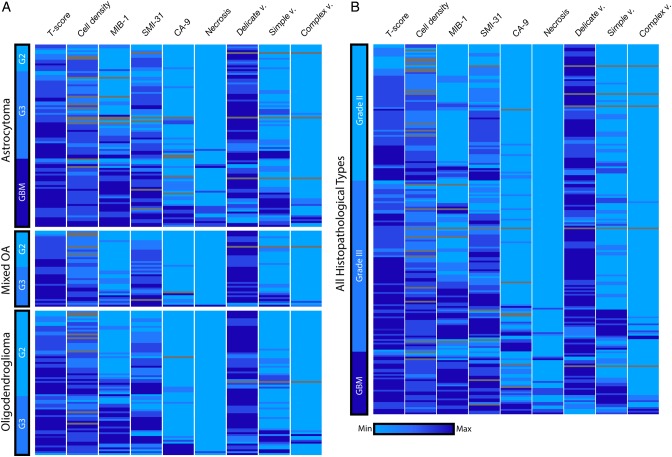
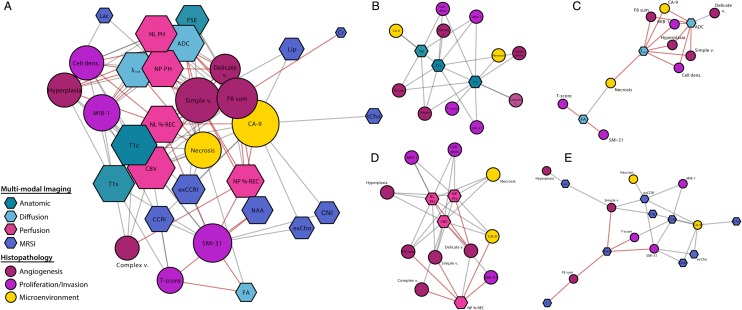
Methods: One hundred and eleven patients previously diagnosed with LGG were scanned at either 1.5 T or 3 T MR at the time of recurrence. Volumetric and intensity parameters were estimated from anatomic, diffusion, perfusion, and metabolic MR data. Direct comparisons of histopathological markers from image-guided tissue samples with metrics derived from the corresponding locations on the in vivo images were made. A bioinformatics approach was applied to visualize and interpret these results, which included imaging heatmaps and network analysis. Multivariate linear-regression modeling was utilized for predicting transformation.
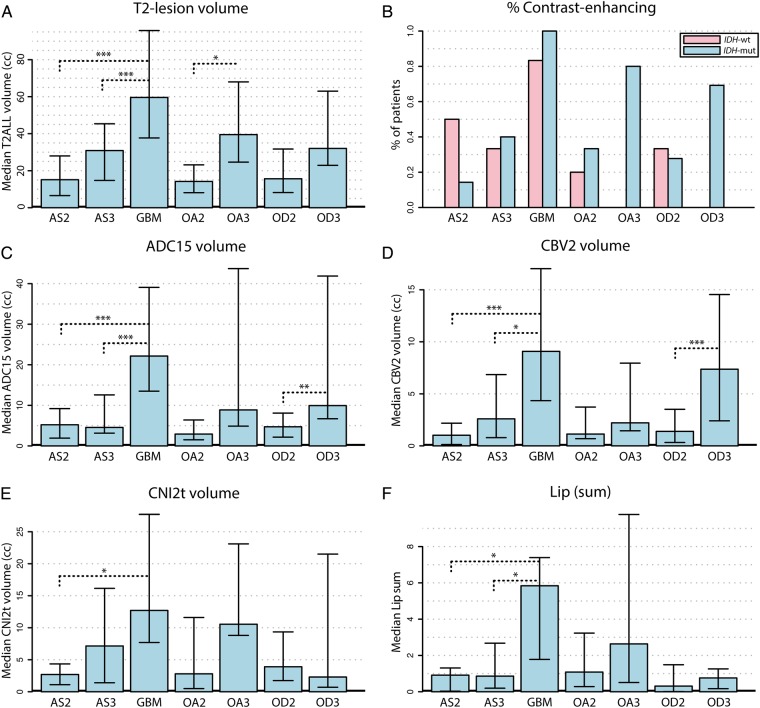
Results: Many advanced imaging parameters were found to be significantly different for patients with tumors that had undergone MT versus those that had not. Imaging metrics calculated at the tissue sample locations highlighted the distinct biological significance of the imaging and the heterogeneity present in recurrent LGG, while multivariate modeling yielded a 76.04% accuracy in predicting MT.
Conclusions: The acquisition and quantitative analysis of such multiparametric MR data may ultimately allow for improved clinical assessment and treatment stratification for patients with recurrent LGG.
Keywords: cancer imaging; low-grade glioma; magnetic resonance; malignant transformation; spectroscopy.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
References
-
- Riemenschneider MJ, Reifenberger G. Molecular neuropathology of low-grade gliomas and its clinical impact. Adv Tech Stand Neurosurg. 2010;35(1):35–64. - PubMed
-
- Grier JT, Batchelor T. Low-grade gliomas in adults. Oncologist. 2006;11(6):681–693. - PubMed
-
- Houillier C, Wang X, Kaloshi G et al. IDH1 or IDH2 mutations predict longer survival and response to temozolomide in low-grade gliomas. Neurology. 2010;75(17):1560–1566. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
