

Increasing follow-up questionnaire response rates in a randomized controlled trial of telehealth for depression: three embedded controlled studies
- PMID: 26912230
- PMCID: PMC4765058
- DOI: 10.1186/s13063-016-1234-3
Increasing follow-up questionnaire response rates in a randomized controlled trial of telehealth for depression: three embedded controlled studies
Abstract
Background: Attrition is problematic in trials, and may be exacerbated in longer studies, telehealth trials and participants with depression - three features of The Healthlines Study. Advance notification, including a photograph and using action-oriented email subject lines might increase response rates, but require further investigation. We examined the effectiveness of these interventions in three embedded Healthlines studies.
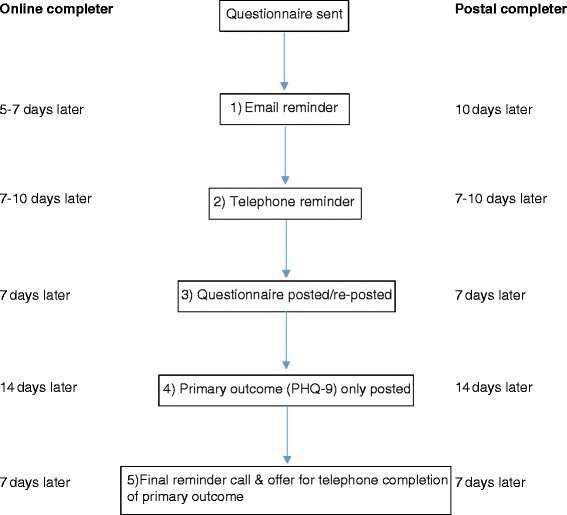
Methods: Based in different trial sites, participants with depression were alternately allocated to be pre-called or not ahead of the 8-month follow-up questionnaire (Study 1), randomized to receive a research team photograph or not with their 12-month questionnaire (Study 2), and randomized to receive an action-oriented ('ACTION REQUIRED') or standard ('Questionnaire reminder') 12-month email reminder (Study 3). Participants could complete online or postal questionnaires, and received up to five questionnaire reminders. The primary outcome was completion of the Patient Health Questionnaire (PHQ-9). Secondary outcome measures were the number of reminders and time to questionnaire completion.
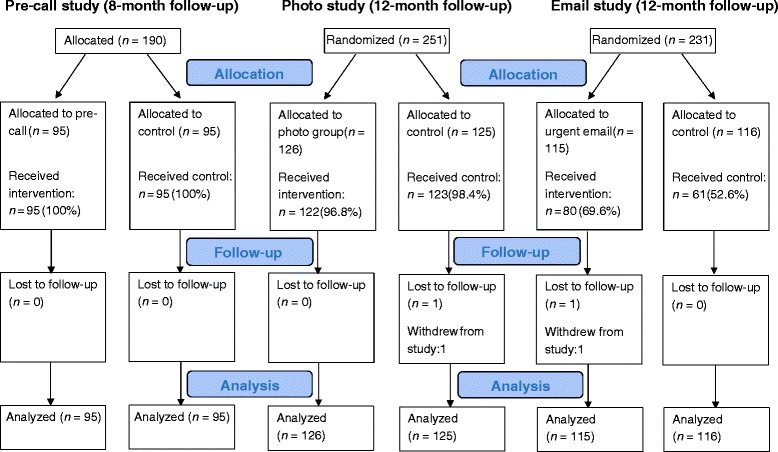
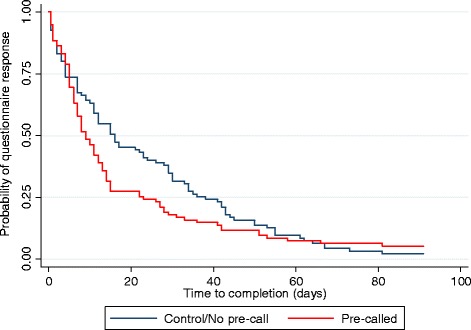
Results: Of a total of 609 Healthlines depression participants, 190, 251 and 231 participants were included in Studies 1-3 (intervention: 95, 126 and 115), respectively. Outcome completion was ≥90 % across studies, with no differences between trial arms (Study 1: OR 0.38, 95 % CI 0.07-2.10; Study 2: OR 0.84, 95 % CI 0.26-2.66; Study 3: OR 0.53 95 % CI 0.19-1.49). Pre-called participants were less likely to require a reminder (48.4 % vs 62.1 %, OR 0.41, 95 % CI 0.21-0.78), required fewer reminders (adjusted difference in means -0.67, 95 % CI -1.13 to -0.20), and completed follow-up quicker (median 8 vs 15 days, HR 1.35, 95 % CI 1.00-1.82) than control subjects. There were no significant between-group differences in Studies 2 or 3.
Conclusions: Eventual response rates in this trial were high, with no further improvement from these interventions. While the photograph and email interventions were ineffective, pre-calling participants reduced time to completion. This strategy might be helpful when the timing of study completion is important. Researchers perceived a substantial benefit from the reduction in reminders with pre-calling, despite no overall decrease in net effort after accounting for pre-notification.
Trial registration: Current Clinical Trials ISRCTN14172341.
Figures
References
-
- Thomas C, Man M, O’Cathain A, Hollinghurst S, Large S, Edwards L, et al. Effectiveness and cost-effectiveness of a telehealth intervention to support the management of long-term conditions: study protocol for two linked randomized controlled trials. Trials. 2014;15:36. doi: 10.1186/1745-6215-15-36. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
