

Motor levels in high cervical spinal cord injuries: Implications for the International Standards for Neurological Classification of Spinal Cord Injury
- PMID: 26913366
- PMCID: PMC5020589
- DOI: 10.1080/10790268.2016.1138602
Motor levels in high cervical spinal cord injuries: Implications for the International Standards for Neurological Classification of Spinal Cord Injury
Abstract
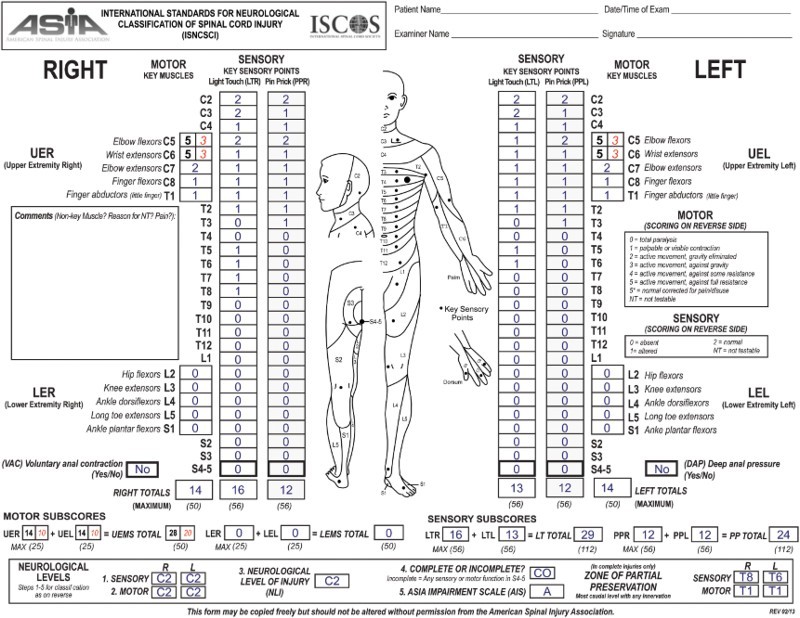
Context/objective: To verify the hypothesis that motor levels (ML) inferred from sensory levels in the upper cervical segments C2-C4 according to the current version of the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) are counterintuitive in cases where the most rostral myotomes C5 and C6 are graded as intact.
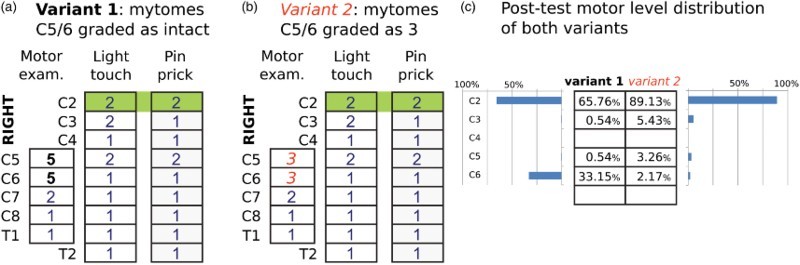
Design: Prospective cohort study of ISNCSCI instructional course participants completing a post-test after the workshop to determine the MLs in two variants of a complete, high cervical spinal cord injury (SCI) case scenario. Both variants were based on the same ISNCSCI sensory and MLs of C2. In the first variant myotomes C5 and C6 were bilaterally graded as intact, while in variant 2 only active movements against gravity were possible (grade 3).
Setting: Eight ISNCSCI instructional courses conducted during the study period from November 2012 until March 2015 in the framework of the European Multicenter Study on Human Spinal Cord Injury (EMSCI- http//emsci.org ).
Participants: Ninety-two clinicians from twenty-two SCI centers. Most of the attendees were physicians (58.7%) or physical therapists (33.7%) and had less than one year (44.6%) experience in SCI medicine.
Interventions: Not applicable.
Outcome measure: The classification performance described as percentage of correctly determined MLs by the clinicians.
Results: Variant 2 (89.13%) was significantly (P < 0.0001) better classified than variant 1 (65.76%). In variant 1 with intact myotomes at C5 and C6, C6 was incorrectly classified as the ML by the clinicians in 33.15% of all cases, whereas in variant 2 with non-intact C5 / C6 myotomes, C6 was rarely chosen (2.17%).
Conclusions: Sensory level deferred MLs in the high cervical region of C2-C4 are counterintuitive whenever the most rostral cervical myotomes are intact. An adjustment of the ML definition in ISNCSCI may be needed.
Keywords: Outcomes research; Recovery of function; Rehabilitation; Spinal cord injuries.
Figures
References
-
- Fawcett JW, Curt A, Steeves JD, Coleman WP, Tuszynski MH, Lammertse D, et al. . Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord 2007;45(3):190–205. doi: 10.1038/sj.sc.3102007 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous