

Early Indicators of Fatal Leptospirosis during the 2010 Epidemic in Puerto Rico
- PMID: 26914210
- PMCID: PMC4767218
- DOI: 10.1371/journal.pntd.0004482
Early Indicators of Fatal Leptospirosis during the 2010 Epidemic in Puerto Rico
Abstract
Background: Leptospirosis is a potentially fatal bacterial zoonosis that is endemic throughout the tropics and may be misdiagnosed as dengue. Delayed hospital admission of leptospirosis patients is associated with increased mortality.
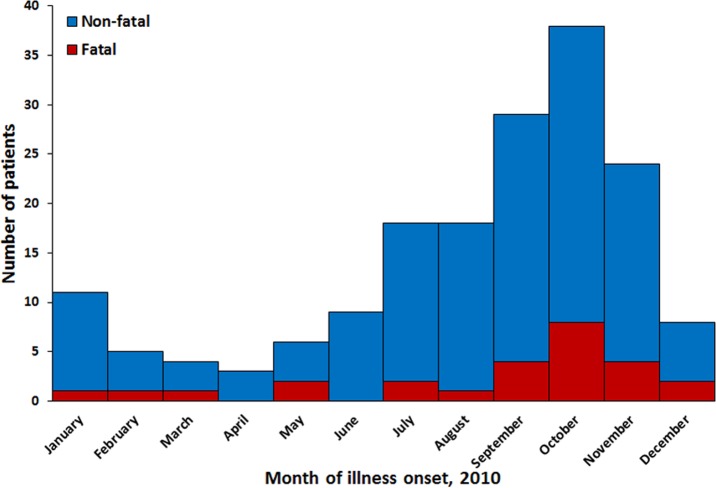
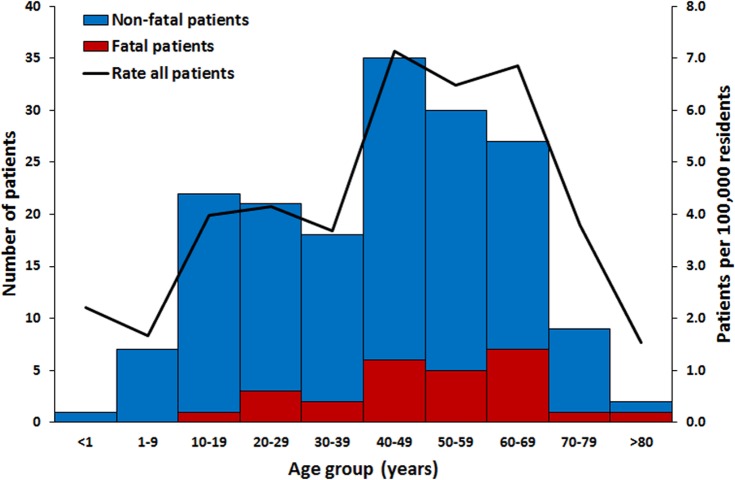
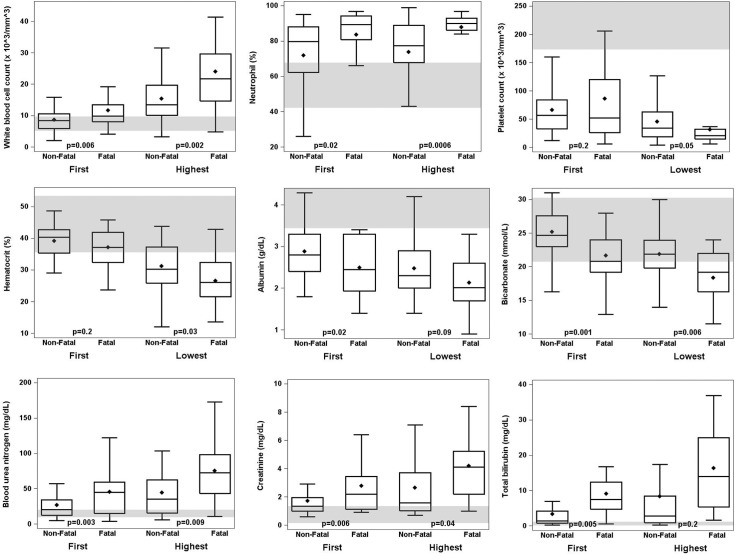
Methodology/principal findings: During a concurrent dengue/leptospirosis epidemic in Puerto Rico in 2010, suspected dengue patients that tested dengue-negative were tested for leptospirosis. Fatal and non-fatal hospitalized leptospirosis patients were matched 1:1-3 by age. Records from all medical visits were evaluated for factors associated with fatal outcome. Among 175 leptospirosis patients identified (4.7 per 100,000 residents), 26 (15%) were fatal. Most patients were older males and had illness onset during the rainy season. Fatal case patients first sought medical care earlier than non-fatal control patients (2.5 vs. 5 days post-illness onset [DPO], p < 0.01), but less frequently first sought care at a hospital (52.4% vs. 92.2%, p < 0.01). Although fatal cases were more often diagnosed with leptospirosis at first medical visit (43.9% vs. 9.6%, p = 0.01), they were admitted to the hospital no earlier than non-fatal controls (4.5 vs. 6 DPO, p = 0.31). Cases less often developed fever (p = 0.03), but more often developed jaundice, edema, leg pain, hemoptysis, and had a seizure (p ≤ 0.03). Multivariable analysis of laboratory values from first medical visit associated with fatal outcome included increased white blood cell (WBC) count with increased creatinine (p = 0.001), and decreased bicarbonate with either increased WBC count, increased creatinine, or decreased platelet count (p < 0.001).
Conclusions/significance: Patients with fatal leptospirosis sought care earlier, but were not admitted for care any earlier than non-fatal patients. Combinations of routine laboratory values predictive of fatal outcome should be considered in admission decision-making for patients with suspected leptospirosis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Yersin C, Bovet P, Merien F, Clement J, Laille M, Van Ranst M, et al. Pulmonary haemorrhage as a predominant cause of death in leptospirosis in Seychelles. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2000;94(1):71–6. Epub 2000/04/05. . - PubMed
-
- Dupont H, Dupont-Perdrizet D, Perie JL, Zehner-Hansen S, Jarrige B, Daijardin JB. Leptospirosis: prognostic factors associated with mortality. Clinical Infectious Diseases. 1997;25(3):720–4. Epub 1997/10/06. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
