

Burden and Prevention of Adverse Cardiac Events in Patients with Concomitant Chronic Heart Failure and Coronary Artery Disease: A Literature Review
- PMID: 26915344
- PMCID: PMC5084727
- DOI: 10.1111/1755-5922.12180
Burden and Prevention of Adverse Cardiac Events in Patients with Concomitant Chronic Heart Failure and Coronary Artery Disease: A Literature Review
Abstract
Background: Chronic heart failure (HF) or coronary artery disease (CAD) confers risk for thromboembolism and secondary adverse cardiac events (ACEs) (e.g., mortality, myocardial infarction, and stroke). When HF and CAD occur concomitantly, ACE risk is reported to be elevated. We investigated ACEs, their epidemiology, and the resulting burden among patients with concomitant HF and CAD through a structured review of recent literature. Antithrombotic treatment for ACE prevention was assessed.
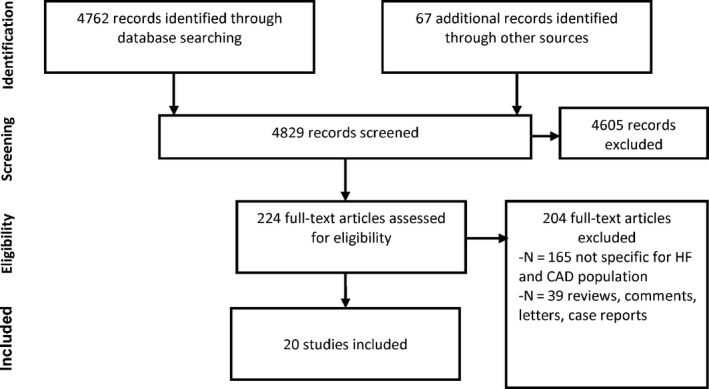
Methods: Pertinent databases (PubMed, other) were searched for relevant articles published from January 2004 to March 2015. Data collected included ACE incidence, healthcare resource use, costs, change in quality of life attributed to ACEs, and treatment practice for prevention of ACEs in patients with concomitant HF and CAD.
Results: Mortality rates for patients with both HF and CAD ranged from 4.9-12.3% at 30 days to 13.7-86% for periods between 9.9 months and 10 years. Incidence of ACEs among HF patients with CAD is, respectively, at least 82% and 15% higher than for patients without HF or without CAD, except for stroke investigated in two studies. All-cause and HF-related hospitalization is the main driver of the economic burden in patients with HF, the majority of whom had CAD origin. Despite high prevalence of ischemic complications, there is limited evidence to support the use of warfarin-type antithrombotics among HF patients.
Conclusion: This study confirms that patients with concomitant HF and CAD are at elevated risk for ACEs and suggests the need for effective new antithrombotic treatments to further decrease ischemic complication rates in this population.
Keywords: Adverse cardiac events; Antithrombotics; Coronary artery disease; Heart failure.
© 2016 John Wiley & Sons Ltd.
References
-
- Liu L, Eisen HJ. Epidemiology of heart failure and scope of the problem. Cardiol Clin 2014;32:1–8. vii. - PubMed
-
- International Diabetes Federation . IDF diabetes atlas, 6th edition. Brussels, Belgium: 2013. http://www.idf.org/diabetesatlas/download-book. (Accessed 6 Jan 2014).
-
- McMurray JJ, Adamopoulos S, Anker SD, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J 2012;33:1787–1847. - PubMed
-
- Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013;34:2949–3003. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
