

Can adverse maternal and perinatal outcomes be predicted when blood pressure becomes elevated? Secondary analyses from the CHIPS (Control of Hypertension In Pregnancy Study) randomized controlled trial
- PMID: 26915709
- PMCID: PMC5021204
- DOI: 10.1111/aogs.12877
Can adverse maternal and perinatal outcomes be predicted when blood pressure becomes elevated? Secondary analyses from the CHIPS (Control of Hypertension In Pregnancy Study) randomized controlled trial
Abstract
Introduction: For women with chronic or gestational hypertension in CHIPS (Control of Hypertension In Pregnancy Study, NCT01192412), we aimed to examine whether clinical predictors collected at randomization could predict adverse outcomes.
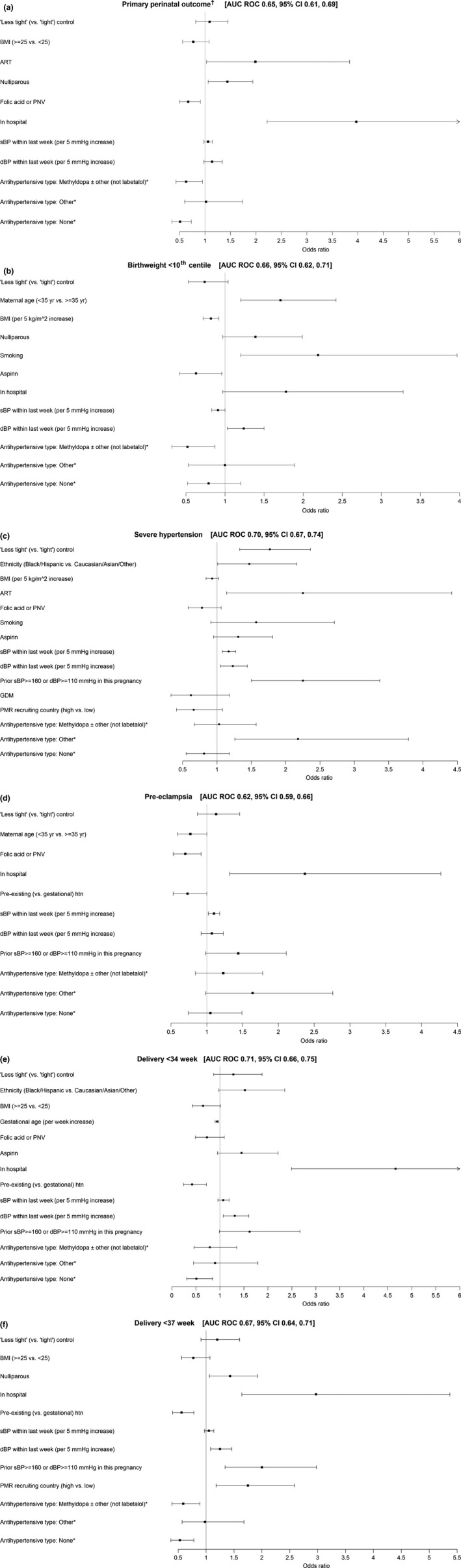
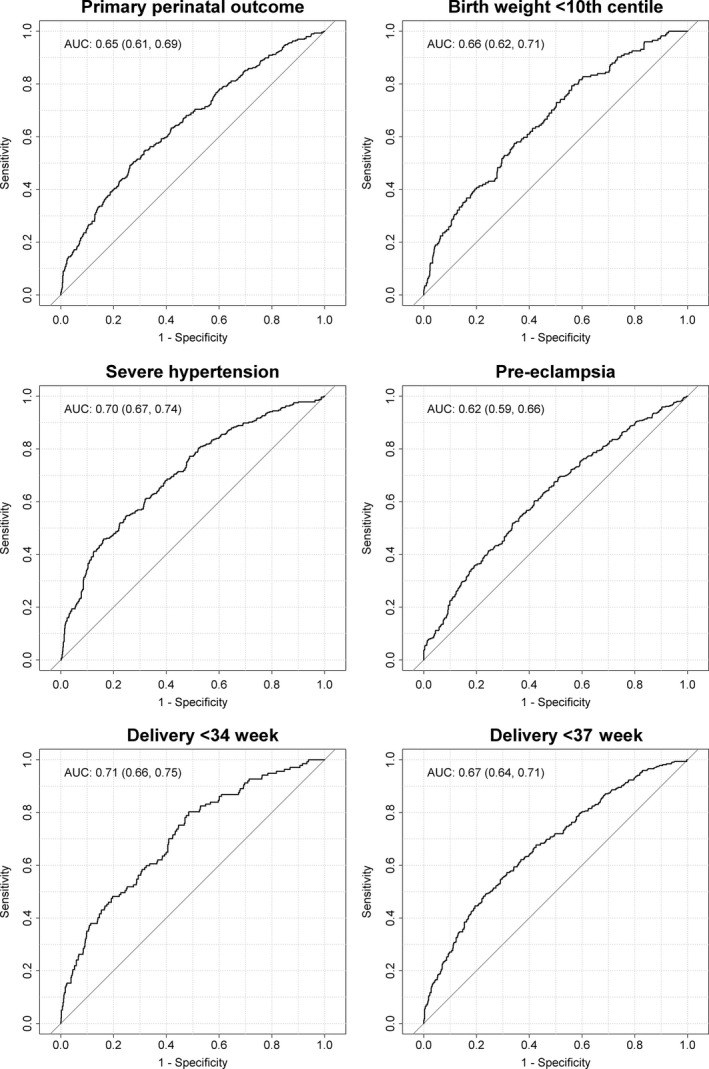
Material and methods: This was a planned, secondary analysis of data from the 987 women in the CHIPS Trial. Logistic regression was used to examine the impact of 19 candidate predictors on the probability of adverse perinatal (pregnancy loss or high level neonatal care for >48 h, or birthweight <10th percentile) or maternal outcomes (severe hypertension, preeclampsia, or delivery at <34 or <37 weeks). A model containing all candidate predictors was used to start the stepwise regression process based on goodness of fit as measured by the Akaike information criterion. For face validity, these variables were forced into the model: treatment group ("less tight" or "tight" control), antihypertensive type at randomization, and blood pressure within 1 week before randomization. Continuous variables were represented continuously or dichotomized based on the smaller p-value in univariate analyses. An area-under-the-receiver-operating-curve (AUC ROC) of ≥0.70 was taken to reflect a potentially useful model.
Results: Point estimates for AUC ROC were <0.70 for all but severe hypertension (0.70, 95% CI 0.67-0.74) and delivery at <34 weeks (0.71, 95% CI 0.66-0.75). Therefore, no model warranted further assessment of performance.
Conclusions: CHIPS data suggest that when women with chronic hypertension develop an elevated blood pressure in pregnancy, or formerly normotensive women develop new gestational hypertension, maternal and current pregnancy clinical characteristics cannot predict adverse outcomes in the index pregnancy.
Keywords: Preexisting hypertension; adverse outcome; chronic hypertension; gestational hypertension; maternal; perinatal; prediction.
© 2016 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Figures
References
-
- von Dadelszen P, Payne B, Li J, Ansermino JM, Broughton PF, Cote AM, et al. Prediction of adverse maternal outcomes in pre‐eclampsia: development and validation of the fullPIERS model. Lancet. 2011;377:219–27. - PubMed
-
- Payne BA, Hutcheon JA, Ansermino JM, Hall DR, Bhutta ZA, Bhutta SZ, et al. A risk prediction model for the assessment and triage of women with hypertensive disorders of pregnancy in low‐resourced settings: the miniPIERS (Pre‐eclampsia Integrated Estimate of RiSk) multi‐country prospective cohort study. PLoS Med. 2014;11:e1001589. - PMC - PubMed
-
- Chappell LC, Duckworth S, Seed PT, Griffin M, Myers J, Mackillop L, et al. Diagnostic accuracy of placental growth factor in women with suspected preeclampsia: a prospective multicenter study. Circulation. 2013;128:2121–31. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
