

Bioengineering the Endocrine Pancreas: Intraomental Islet Transplantation Within a Biologic Resorbable Scaffold
- PMID: 26916086
- PMCID: PMC5384628
- DOI: 10.2337/db15-1525
Bioengineering the Endocrine Pancreas: Intraomental Islet Transplantation Within a Biologic Resorbable Scaffold
Abstract
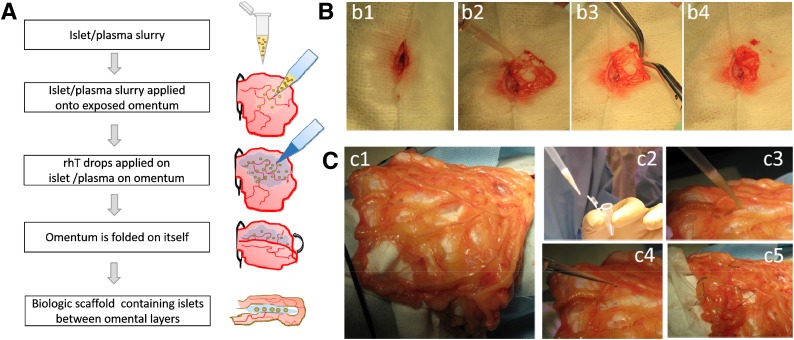
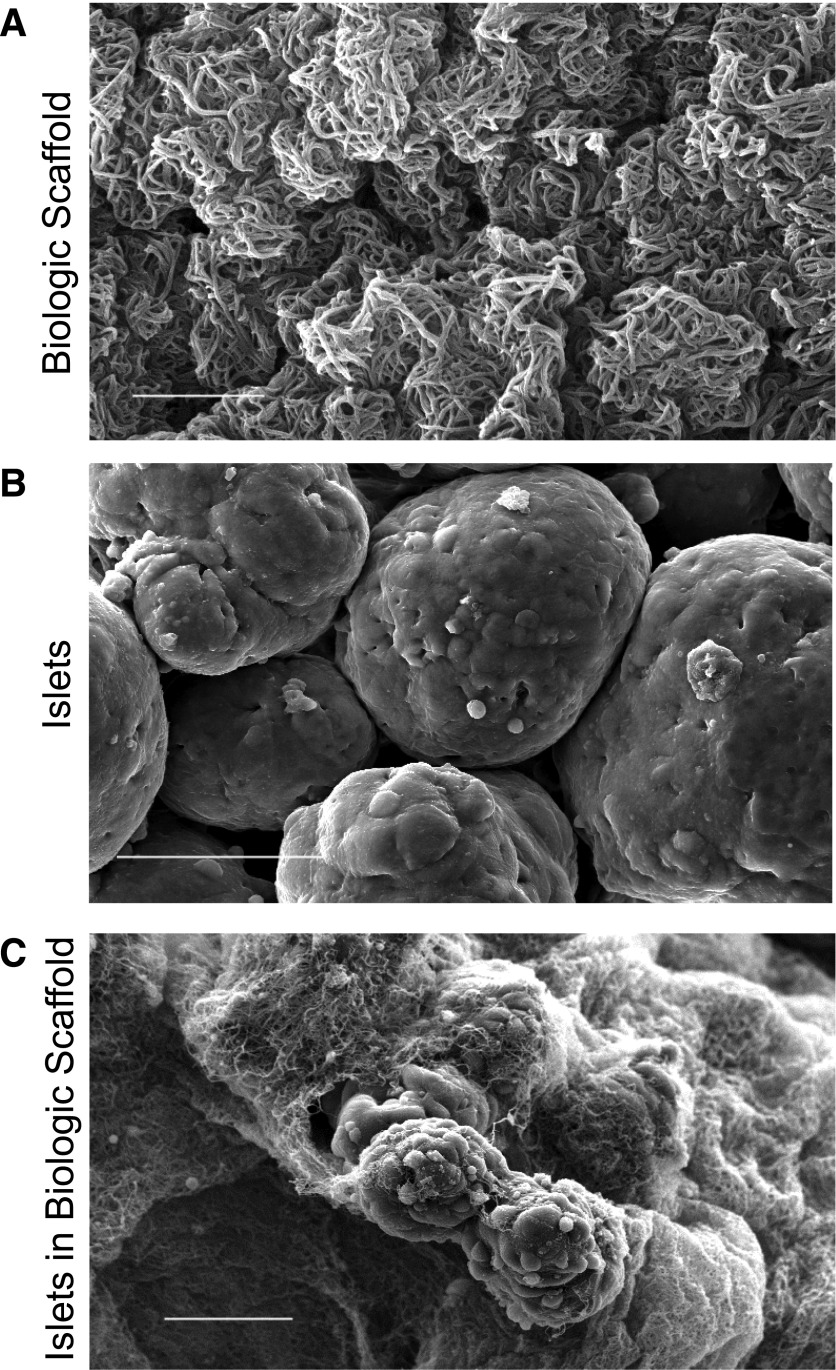
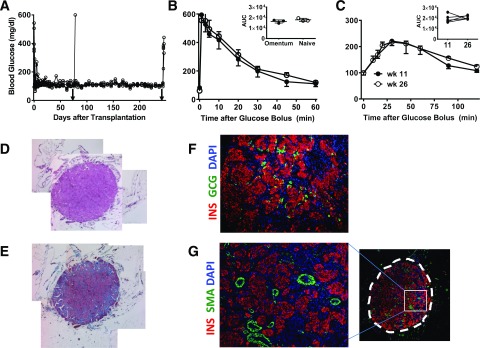
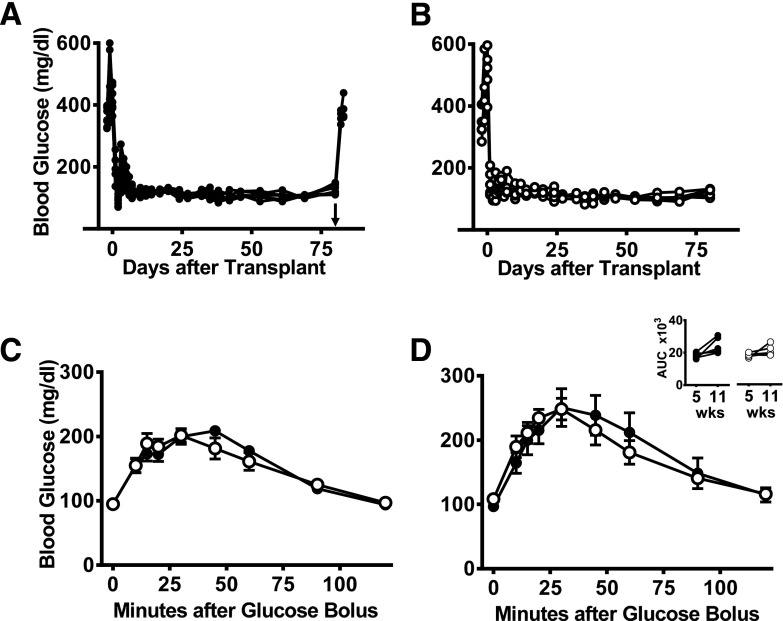
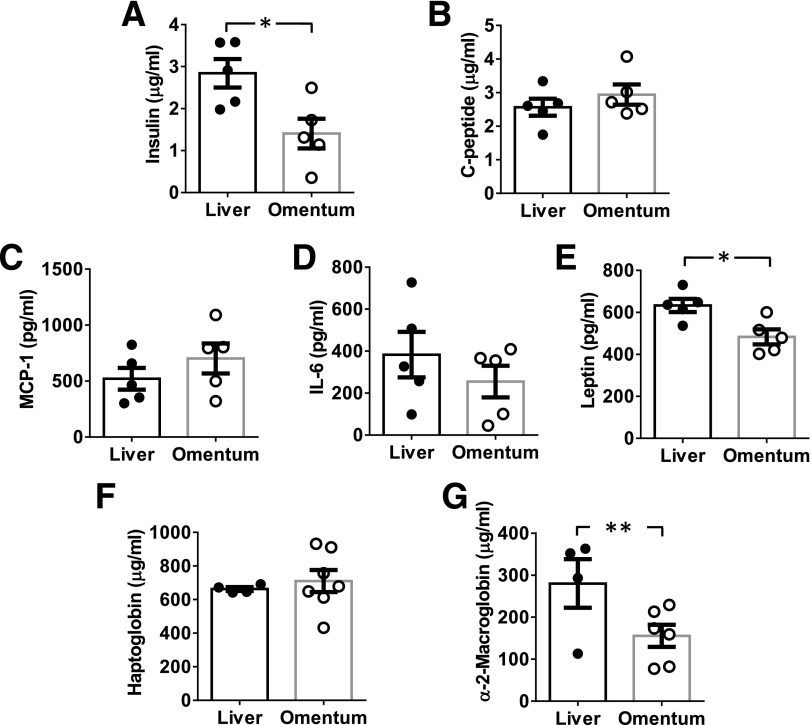
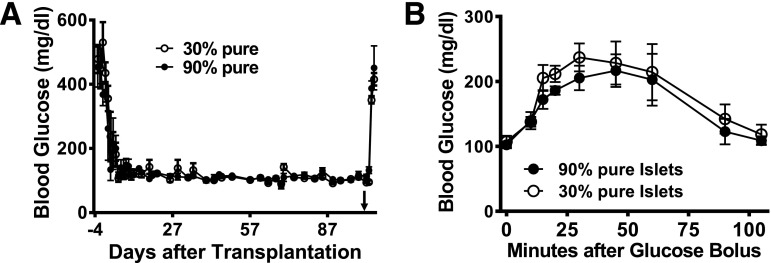
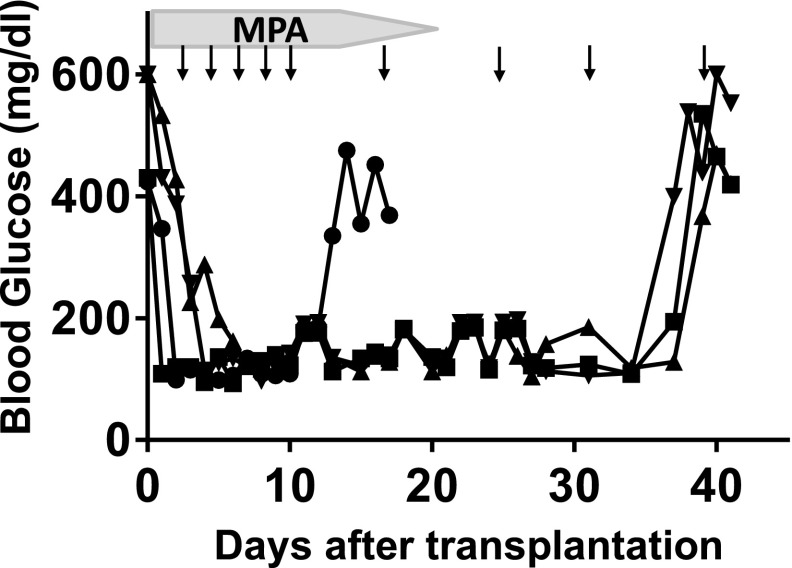
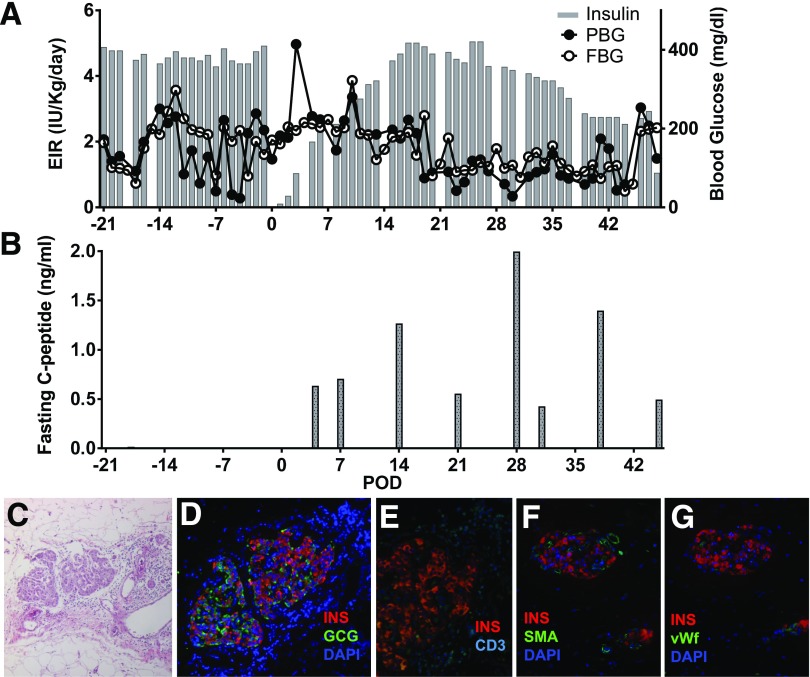
Transplantation of pancreatic islets is a therapeutic option to preserve or restore β-cell function. Our study was aimed at developing a clinically applicable protocol for extrahepatic transplantation of pancreatic islets. The potency of islets implanted onto the omentum, using an in situ-generated adherent, resorbable plasma-thrombin biologic scaffold, was evaluated in diabetic rat and nonhuman primate (NHP) models. Intraomental islet engraftment in the biologic scaffold was confirmed by achievement of improved metabolic function and preservation of islet cytoarchitecture, with reconstitution of rich intrainsular vascular networks in both species. Long-term nonfasting normoglycemia and adequate glucose clearance (tolerance tests) were achieved in both intrahepatic and intraomental sites in rats. Intraomental graft recipients displayed lower levels of serum biomarkers of islet distress (e.g., acute serum insulin) and inflammation (e.g., leptin and α2-macroglobulin). Importantly, low-purity (30:70% endocrine:exocrine) syngeneic rat islet preparations displayed function equivalent to that of pure (>95% endocrine) preparations after intraomental biologic scaffold implantation. Moreover, the biologic scaffold sustained allogeneic islet engraftment in immunosuppressed recipients. Collectively, our feasibility/efficacy data, along with the simplicity of the procedure and the safety of the biologic scaffold components, represented sufficient preclinical testing to proceed to a pilot phase I/II clinical trial.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Pileggi A, Ricordi C, Kenyon NS, et al. . Twenty years of clinical islet transplantation at the Diabetes Research Institute--University of Miami. Clin Transpl 2004;177–204 - PubMed
-
- Bennet W, Groth CG, Larsson R, Nilsson B, Korsgren O. Isolated human islets trigger an instant blood mediated inflammatory reaction: implications for intraportal islet transplantation as a treatment for patients with type 1 diabetes. Ups J Med Sci 2000;105:125–133 - PubMed
-
- Moberg L, Johansson H, Lukinius A, et al. . Production of tissue factor by pancreatic islet cells as a trigger of detrimental thrombotic reactions in clinical islet transplantation. Lancet 2002;360:2039–2045 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
