

Percent reduction in LDL cholesterol following high-intensity statin therapy: potential implications for guidelines and for the prescription of emerging lipid-lowering agents
- PMID: 26916794
- PMCID: PMC4852064
- DOI: 10.1093/eurheartj/ehw046
Percent reduction in LDL cholesterol following high-intensity statin therapy: potential implications for guidelines and for the prescription of emerging lipid-lowering agents
Abstract
Aims: Current statin guidelines in Europe and Canada advocate achieving a fixed LDL target or the attainment of a ≥50% reduction in low-density lipoprotein cholesterol (LDLC), while current US guidelines advocate the use of statin therapies that reduce LDLC by <50% (moderate intensity) or ≥50% (high intensity). Data are limited, however, linking the achievement of these % reduction thresholds to subsequent cardiovascular outcomes particularly for contemporary high-intensity regimens.
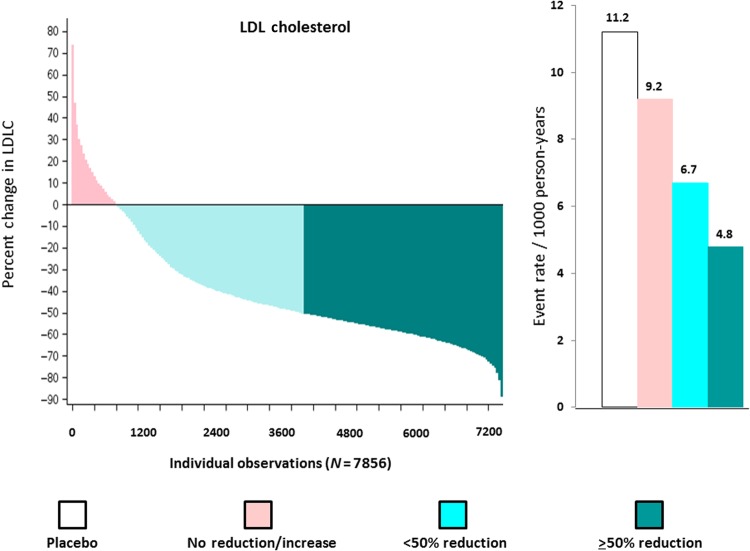
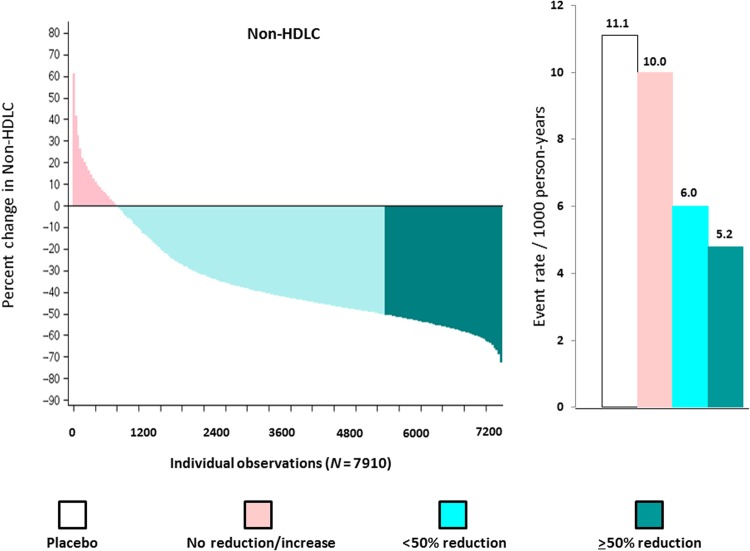
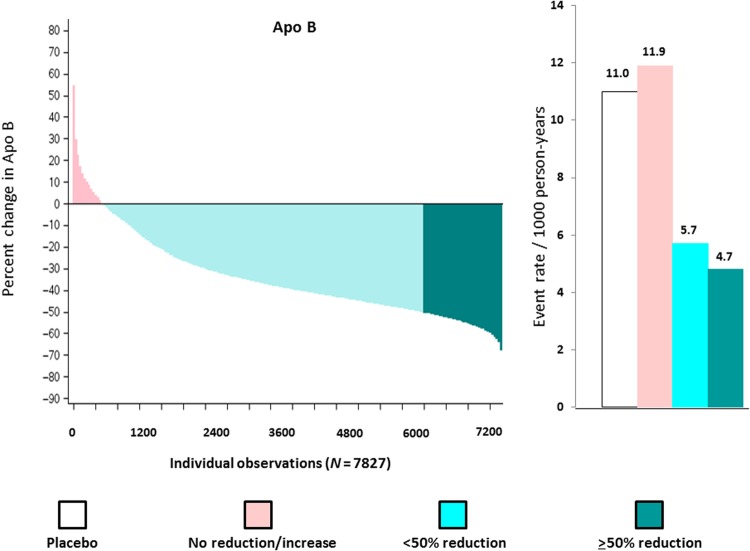
Methods and results: In a randomized trial of 17 082 initially healthy men and women with median baseline LDLC of 108 mg/dL (interquartile range 94-119), we (i) used waterfall plots to assess the variability in LDLC response to rosuvastatin 20 mg daily and (ii) evaluated the impact of reaching ≥50% reductions in LDLC on risk of developing the first cardiovascular events. Among rosuvastatin allocated participants, 3640 individuals (46.3%) experienced an LDLC reduction ≥50%; 3365 individuals (42.8%) experienced an LDLC reduction >0 but <50%; and 851 individuals (10.8%) experienced no reduction or an increase in LDLC compared with baseline. These % LDLC reductions directly related to the risks of first cardiovascular events; at trial completion, incidence rates for the primary endpoint were 11.2, 9.2, 6.7, and 4.8 per 1000 person-years for those in the placebo, no LDLC reduction, LDLC reduction <50%, and LDLC reduction ≥50% groups, respectively. Compared with placebo, the multivariable adjusted hazard ratios for sequentially greater on-treatment per cent reductions in LDLC were 0.91 (95%CI 0.54-1.53), 0.61 (95%CI 0.44-0.83), and 0.43 (95%CI 0.30-0.60) (P < 0.00001). Similar relationships between % reduction and clinical outcomes were observed in analyses focusing on non-HDLC or apolipoprotein B.
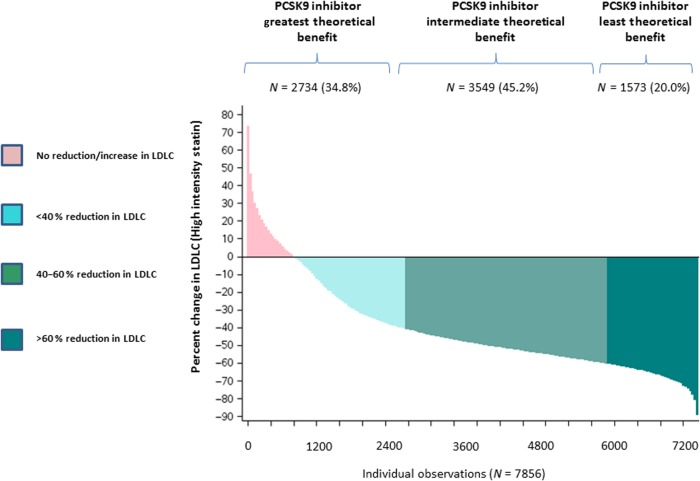
Conclusions: As documented for low- and moderate-intensity regimens, variability in % LDLC reduction following high-intensity statin therapy is wide yet the magnitude of this % reduction directly relates to efficacy. These data support guideline approaches that incorporate % reduction targets for statin therapy as well as absolute targets, and might provide a structure for the allocation of emerging adjunctive lipid-lowering therapies such as PCSK9 inhibitors should these agents prove broadly effective for cardiovascular event reduction.
Keywords: Apolipoprotein B; Guidelines; LDLC; PCSK9; Prevention; Statin therapy.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
Comment in
-
Lower might be better - It matters how you get there, and in whom.Eur Heart J. 2016 May 1;37(17):1380-3. doi: 10.1093/eurheartj/ehw102. Epub 2016 Mar 29. Eur Heart J. 2016. PMID: 27026749 No abstract available.
References
-
- Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, Albus C, Benlian P, Boysen G, Cifkova R, Deaton C, Ebrahim S, Fisher M, Germano G, Hobbs R, Hoes A, Karadeniz S, Mezzani A, Prescott E, Ryden L, Scherer M, Syvane M, Scholte op Remier WJ, Vrints C, Wood D, Zamorano JL, Zannad F. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). Eur Heart J 2012;33:1635–1701. - PubMed
-
- Anderson TJ, Grégoire J, Hegele RA, Couture P, Mancini GB, McPherson R, Francis GA, Poirier P, Lau DC, Grover S, Genest J Jr, Carpentier AC, Dufour R, Gupta M, Ward R, Leiter LA, Lonn E, Ng DS, Pearson GJ, Yates GM, Stone JA, Ur E. 2012 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol 2013;29:151–167. - PubMed
-
- Stone NJ, Robinson J, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC, Watson K, Wilson PWF. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2889–2934. - PubMed
-
- Boekholdt SM, Hovingh GK, Mora S, Arsenault BJ, Amerenco P, Pedersen TR, LaRosa JC, Waters DD, DeMicco DA, Simes RJ, Keech AC, Colquhoun D, Hitman GA, Betteridge DJ, Clearfield MB, Downs JR, Colhoun HM, Gotto AM, Ridker PM, Grundy SM, Kastelein JJP. Very low levels of atherogenic lipoproteins and the risk for cardiovascular events. A meta-analysis of statin trials. J Am Coll Cardiol 2014;64:485–494. - PMC - PubMed
-
- Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008;359:2195–2207. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
