

Preterm Versus Term Children: Analysis of Sedation/Anesthesia Adverse Events and Longitudinal Risk
- PMID: 26917674
- PMCID: PMC9923625
- DOI: 10.1542/peds.2015-0463
Preterm Versus Term Children: Analysis of Sedation/Anesthesia Adverse Events and Longitudinal Risk
Abstract
Background and objectives: Preterm and former preterm children frequently require sedation/anesthesia for diagnostic and therapeutic procedures. Our objective was to determine the age at which children who are born <37 weeks gestational age are no longer at increased risk for sedation/anesthesia adverse events. Our secondary objective was to describe the nature and incidence of adverse events.
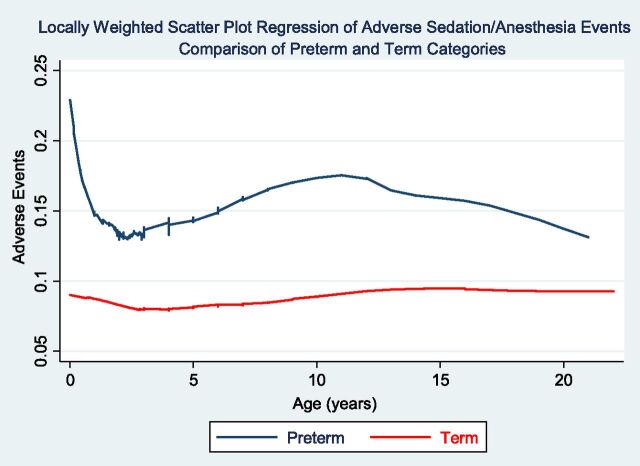
Methods: This is a prospective observational study of children receiving sedation/anesthesia for diagnostic and/or therapeutic procedures outside of the operating room by the Pediatric Sedation Research Consortium. A total of 57,227 patients 0 to 22 years of age were eligible for this study. All adverse events and descriptive terms were predefined. Logistic regression and locally weighted scatterplot regression were used for analysis.
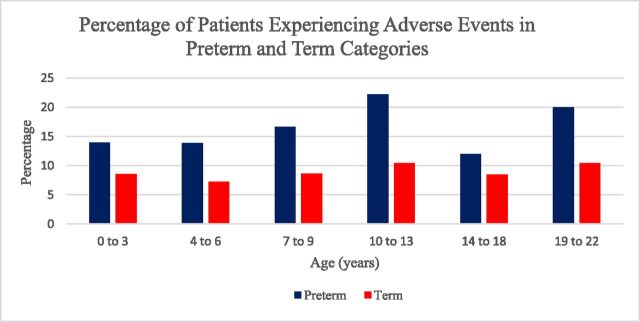
Results: Preterm and former preterm children had higher adverse event rates (14.7% vs 8.5%) compared with children born at term. Our analysis revealed a biphasic pattern for the development of adverse sedation/anesthesia events. Airway and respiratory adverse events were most commonly reported. MRI scans were the most commonly performed procedures in both categories of patients.
Conclusions: Patients born preterm are nearly twice as likely to develop sedation/anesthesia adverse events, and this risk continues up to 23 years of age. We recommend obtaining birth history during the formulation of an anesthetic/sedation plan, with heightened awareness that preterm and former preterm children may be at increased risk. Further prospective studies focusing on the etiology and prevention of adverse events in former preterm patients are warranted.
Copyright © 2016 by the American Academy of Pediatrics.
Conflict of interest statement
Figures
Comment in
-
The Use of Patient Registries to Detect Risk Factors of Anesthesia and Sedation Complications.Pediatrics. 2016 Mar;137(3):e20154579. doi: 10.1542/peds.2015-4579. Epub 2016 Feb 25. Pediatrics. 2016. PMID: 26917673 No abstract available.
References
-
- Centers for Disease Control and Prevention;Preterm birth . Available at: www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm. Accessed April 16, 2014
-
- Cohen MM, Cameron CB, Duncan PG. Pediatric anesthesia morbidity and mortality in the perioperative period. Anesth Analg. 1990;70(2):160–167 - PubMed
-
- Keenan RL, Shapiro JH, Dawson K. Frequency of anesthetic cardiac arrests in infants: effect of pediatric anesthesiologists. J Clin Anesth. 1991;3(6):433–437 - PubMed
-
- Lee C, Mason L. Complications in paediatric anaesthesia. Curr Opin Anaesthesiol. 2006;19(3):262–267 - PubMed
-
- Litman RS, Soin K, Salam A. Chloral hydrate sedation in term and preterm infants: an analysis of efficacy and complications. Anesth Analg. 2010;110(3):739–746 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
