

Evaluation of Aortic Blood Flow and Wall Shear Stress in Aortic Stenosis and Its Association With Left Ventricular Remodeling
- PMID: 26917824
- PMCID: PMC4772425
- DOI: 10.1161/CIRCIMAGING.115.004038
Evaluation of Aortic Blood Flow and Wall Shear Stress in Aortic Stenosis and Its Association With Left Ventricular Remodeling
Abstract
Background: Aortic stenosis (AS) leads to variable stress for the left ventricle (LV) and consequently a broad range of LV remodeling. The aim of this study was to describe blood flow patterns in the ascending aorta of patients with AS and determine their association with remodeling.
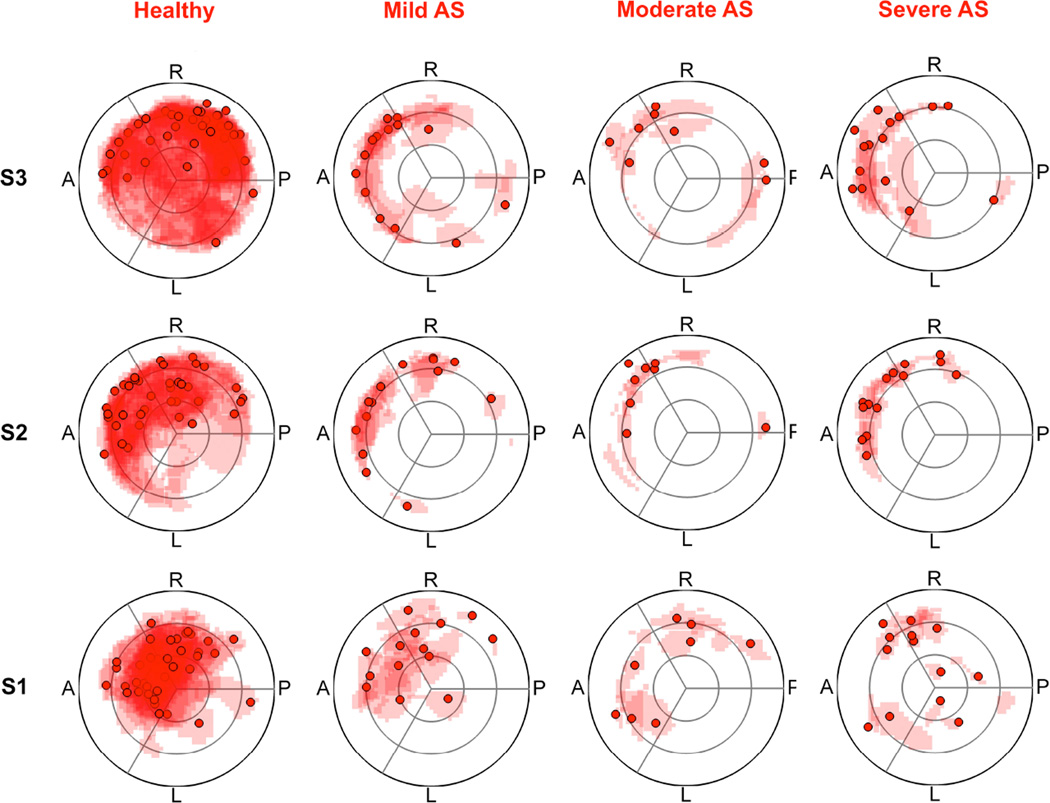
Methods and results: Thirty-seven patients with AS (14 mild, 8 moderate, 15 severe; age, 63±13 years) and 37 healthy controls (age, 60±10 years) underwent 4-dimensional-flow magnetic resonance imaging. Helical and vortical flow formations and flow eccentricity were assessed in the ascending aorta. Normalized flow displacement from the vessel center and peak systolic wall shear stress in the ascending aorta were quantified. LV remodeling was assessed based on LV mass index and the ratio of LV mass:end-diastolic volume (relative wall mass). Marked helical and vortical flow formation and eccentricity were more prevalent in patients with AS than in healthy subjects, and patients with AS exhibited an asymmetrical and elevated distribution of peak systolic wall shear stress. In AS, aortic orifice area was strongly negatively associated with vortical flow formation (P=0.0274), eccentricity (P=0.0070), and flow displacement (P=0.0021). Bicuspid aortic valve was associated with more intense helical (P=0.0098) and vortical flow formation (P=0.0536), higher flow displacement (P=0.11), and higher peak systolic wall shear stress (P=0.0926). LV mass index and relative wall mass were significantly associated with aortic orifice area (P=0.0611, P=0.0058) and flow displacement (P=0.0058, P=0.0283).
Conclusions: In this pilot study, AS leads to abnormal blood flow pattern and peak systolic wall shear stress in the ascending aorta. In addition to aortic orifice area, normalized flow displacement was significantly associated with LV remodeling.
Keywords: aorta; aortic valve stenosis; heart valve diseases; heart ventricles; magnetic resonance imaging.
© 2016 American Heart Association, Inc.
Figures




Comment in
-
Valve, Ventricle, and Vessel: The Triumvirate of Aortic Stenosis Assessment.Circ Cardiovasc Imaging. 2016 Mar;9(3):e004590. doi: 10.1161/CIRCIMAGING.116.004590. Circ Cardiovasc Imaging. 2016. PMID: 26917825 No abstract available.
References
-
- Pibarot P, Dumesnil JG. Improving assessment of aortic stenosis. J Am Coll Cardiol. 2012;60:169–180. - PubMed
-
- Joint Task Force on the Management of Valvular Heart Disease of the European Society of C, European Association for Cardio-Thoracic S. Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, Borger MA, Carrel TP, De Bonis M, Evangelista A, Falk V, Iung B, Lancellotti P, Pierard L, Price S, Schafers HJ, Schuler G, Stepinska J, Swedberg K, Takkenberg J, Von Oppell UO, Windecker S, Zamorano JL, Zembala M. Guidelines on the management of valvular heart disease (version 2012) Eur Heart J. 2012;33:2451–2496. - PubMed
-
- Dweck MR, Joshi S, Murigu T, Gulati A, Alpendurada F, Jabbour A, Maceira A, Roussin I, Northridge DB, Kilner PJ, Cook SA, Boon NA, Pepper J, Mohiaddin RH, Newby DE, Pennell DJ, Prasad SK. Left ventricular remodeling and hypertrophy in patients with aortic stenosis: Insights from cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2012;14:50. - PMC - PubMed
-
- Dweck MR, Boon NA, Newby DE. Calcific aortic stenosis: A disease of the valve and the myocardium. J Am Coll Cardiol. 2012;60:1854–1863. - PubMed
-
- Cioffi G, Faggiano P, Vizzardi E, Tarantini L, Cramariuc D, Gerdts E, de Simone G. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart. 2011;97:301–307. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
