

Case Reports
doi: 10.4103/0972-3919.172361.
Great cervical venous tumoral thrombosis of melanotic medullary carcinoma thyroid: Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography enabled diagnosis and radiotherapy planning
Affiliations
- PMID: 26917895
- PMCID: PMC4746842
- DOI: 10.4103/0972-3919.172361
Item in Clipboard
Case Reports
Great cervical venous tumoral thrombosis of melanotic medullary carcinoma thyroid: Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography enabled diagnosis and radiotherapy planning
Indian J Nucl Med.
2016 Jan-Mar.
Abstract
The authors report an extremely rare occurrence of a massive tumor thrombus involving right internal and external jugular veins extending into superior vena cava from a still rarer melanotic medullary carcinoma thyroid in the postoperative follow-up. The case was managed by hypofractionated intensity modulated radiotherapy technique with gratifying results.
Keywords: Hypofractionated radiotherapy; intensity modulated radiotherapy; melanotic medullary carcinoma thyroid; tumor thrombus.
Figures

(a) Gross specimen showing nodular enlargement of thyroid with blackish discoloration of the right lobe. (b) Microscopic features showing polygonal to spindle cells, in an organoid pattern with clumped chromatin, abundant cytoplasm, and areas of necrosis, focal hemorrhage, copious extracellular brownish black melanin pigment (arrow). (c) Immunohistochemistry right lobe shows tumor cells with brownish-black pigment showing strong cytoplasmic positivity with HMB45. (d) Immunohistochemistry left lobe shows tumor cells with brownish-black pigment showing strong cytoplasmic positivity with calcitonin

Coronal and axial section of fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography showing intensely hypermetabolic hypo dense intraluminal filling defect right internal jugular vein, external jugular vein, subclavian vein confluencing at the right innominate vein with inferior extension into superior vena cava (arrow) and a small metabolically active pretracheal lymph node (dotted arrow)

Coronal fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography postradiotherapy showing complete metabolic regression in the intravascular tumor (arrow) with significant reduction in the tumor thrombus load and better contrast passage through the superior vena cava (dotted arrow)

Color Doppler of the neck showing grossly shrunken thrombus in the right internal jugular vein with absent flow (arrow) and normal flow through the left innominate vein (dotted arrow)
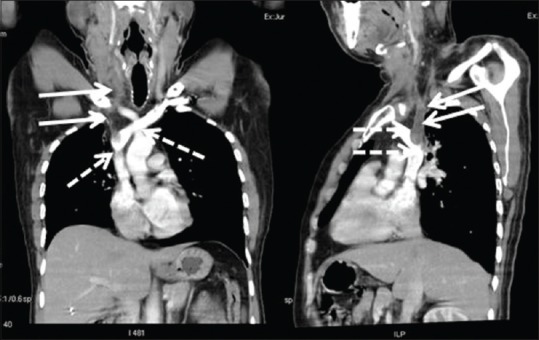
Coronal and sagittal contrast computed tomography chest showing hypodense filling defect in the right internal jugular vein reduced in extent with tiny calcifications, suggesting chronic thrombus (arrows), and patent left innominate vein filled with contrast streaking past the thrombus into superior vena cava (dotted arrows)
References
-
- Singh ZN, Ray R, Kumar N, Aron M, Gupta SD. Medullary thyroid carcinoma with melanin production – A case report. Indian J Pathol Microbiol. 1999;42:159–63. - PubMed
-
- Uribe M, Fenoglio-Preiser CM, Grimes M, Feind C. Medullary carcinoma of the thyroid gland. Clinical, pathological, and immunohistochemical features with review of the literature. Am J Surg Pathol. 1985;9:577–94. - PubMed
-
- Moley JF, Debenedetti MK, Dilley WG, Tisell LE, Wells SA. Surgical management of patients with persistent or recurrent medullary thyroid cancer. J Intern Med. 1998;243:521–6. - PubMed
-
- Evans DB, Fleming JB, Lee JE, Cote G, Gagel RF. The surgical treatment of medullary thyroid carcinoma. Semin Surg Oncol. 1999;16:50–63. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
