

Is C-reactive protein the single most useful predictor of difficult laparoscopic cholecystectomy or its conversion? A pilot study
- PMID: 26917916
- PMCID: PMC4746971
- DOI: 10.4103/0972-9941.158963
Is C-reactive protein the single most useful predictor of difficult laparoscopic cholecystectomy or its conversion? A pilot study
Abstract
Introduction: Both converted and difficult laparoscopic cholecystectomies (LC) have impact on operating time and training of juniors. The aim of this study is to evaluate parameters that predict difficult LC or conversion (C), and find predictive values for different cut-off points of C-reactive protein (CRP) for conversion.
Materials and methods: A retrospective cohort study of cholecystectomies performed from January 2011 to December 2012 at NHS trust was undertaken. Association of intra-operative difficulties or conversion with the following factors was studied: Age, gender, CRP, white blood cell count (WBC), history of pancreatitis, and endoscopic retrograde cholangiopancreatography (ERCP).
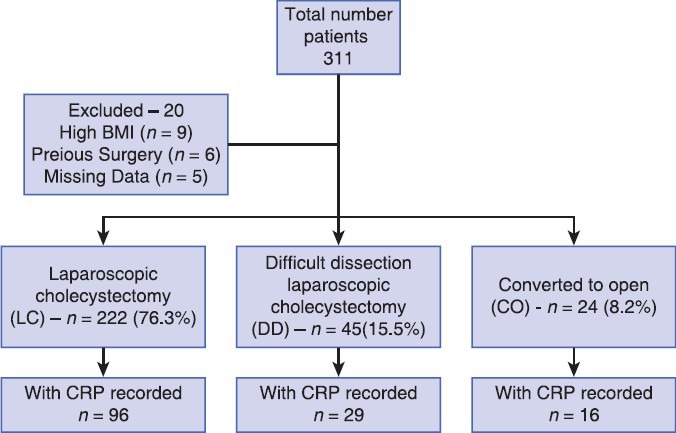
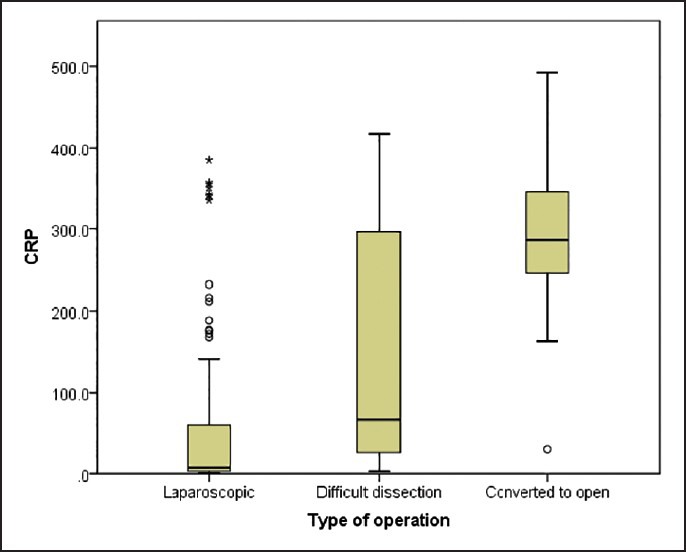
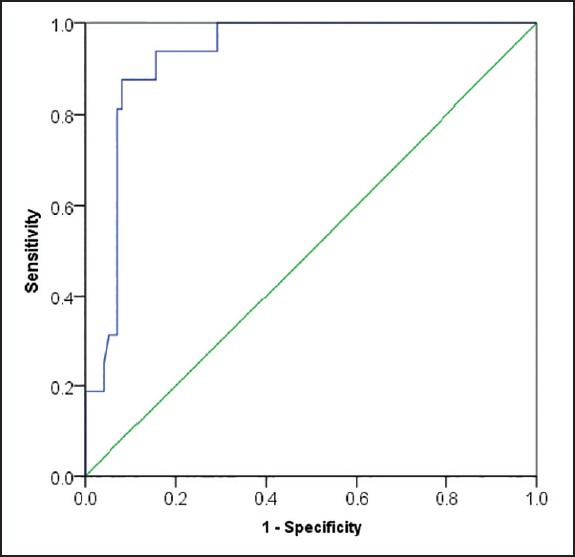
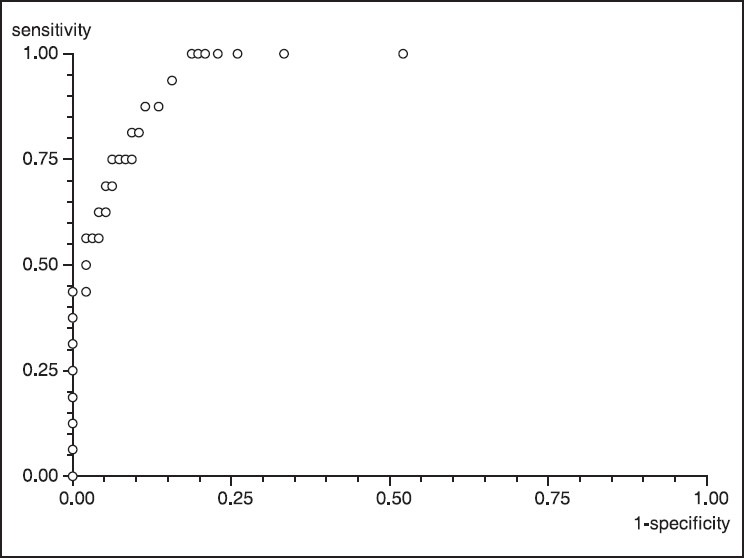
Results: Two hundred and ninety one patients were analysed (222 laparoscopic, 45 difficult LC and 24 C). Only 141 patients had a recorded CRP. Median CRP was highest for patients who were converted (286.20) compared to those who had difficult LC (67.40) or LC (7.05). Those patients who did not have preoperative CRP (8/150, 5.3%) had less chance of conversion than those who had CRP (16/141, 11.34%) (P = 0.063). Patients with CRP of ≤220 (3/91, 3.2%) had significantly less chance of conversion than those with CRP >220 (13/21, 61.9%) (P < 0.001). High preoperative CRP, WBC count and ERCP, were predictors of conversion. These factors were only marginally better than CRP alone in predicting conversion.
Conclusion: CRP can be a strong predictor of conversion of LC. Further validation of the results is needed.
Keywords: C-reactive protein; difficult dissection; laparoscopic cholecystectomy; predicting conversion.
Conflict of interest statement
Figures
References
-
- Giger UF, Michel JM, Opitz I, Th Inderbitzin D, Kocher T, Krähenbühl L, et al. Risk factors for perioperative complications in patients undergoing laparoscopic cholecystectomy: Analysis of 22,953 consecutive cases from the Swiss Association of Laparoscopic and Thoracoscopic Surgery database. J Am Coll Surg. 2006;203:723–8. - PubMed
-
- Sharma SK, Thapa PB, Pandey A, Kayastha B, Poudyal S, Uprety KR, et al. Predicting difficulties during laparoscopic cholecystectomy by preoperative ultrasound. Kathmandu Univ Med J (KUMJ) 2007;5:8–11. - PubMed
-
- Târcoveanu E, Niculescu D, Georgescu S, Epure O, Bradea C. Conversion in laparoscopic cholecystectomy. Chirurgia (Bucur) 2005;100:437–44. - PubMed
-
- Tayeb M, Raza SA, Khan MR, Azami R. Conversion from laparoscopic to open cholecystectomy: Multivariate analysis of preoperative risk factors. J Postgrad Med. 2005;51:17–20. - PubMed
-
- Ilie AC, Nica C, Szucsik IA, Motoc A, Sava A, Grosu S. Preoperative ultrasonography as a mean of predicting the conversion of mini cholecystectomy into classic cholecystectomy. Rev Med Chir Soc Med Nat Iasi. 2009;113:1136–40. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous