

Pharmacokinetics of Rilpivirine in HIV-Infected Pregnant Women
- PMID: 26918544
- PMCID: PMC4911231
- DOI: 10.1097/QAI.0000000000000968
Pharmacokinetics of Rilpivirine in HIV-Infected Pregnant Women
Abstract
Background: Rilpivirine pharmacokinetics is defined by its absorption, distribution, metabolism, and excretion. Pregnancy can affect these factors by changes in cardiac output, protein binding, volume of distribution, and cytochrome P450 (CYP) 3A4 activity. Rilpivirine is metabolized by CYP3A4. The impact of pregnancy on rilpivirine pharmacokinetics is largely unknown.
Methods: International Maternal Pediatric Adolescent AIDS Clinical Trials P1026s is a multicenter, nonblinded, prospective study evaluating antiretroviral pharmacokinetics in HIV-infected pregnant women that included a cohort receiving rilpivirine 25 mg once daily as part of their combination antiretrovirals for clinical care. Thirty-two women were enrolled in this study. Intensive pharmacokinetic sampling was performed at steady state during the second trimester, the third trimester, and postpartum. Maternal and umbilical cord blood samples were obtained at delivery. Plasma rilpivirine concentration was measured using liquid chromatography-mass spectrometry; lower limit of quantitation was 10 ng/mL.
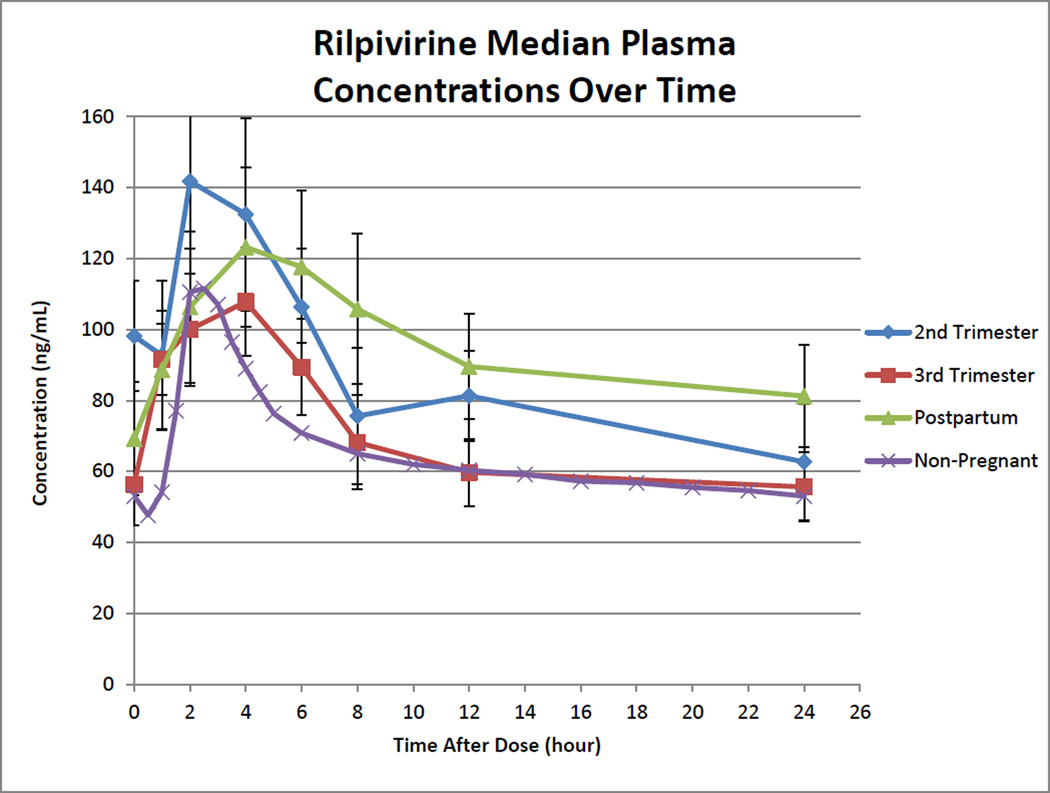
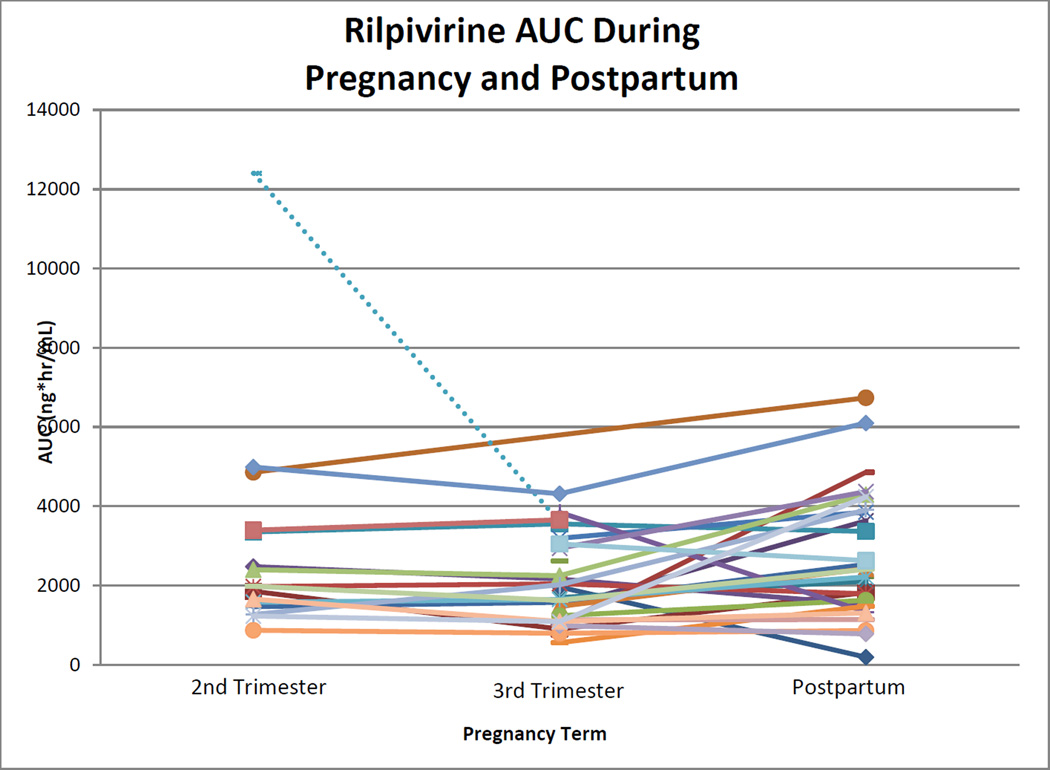
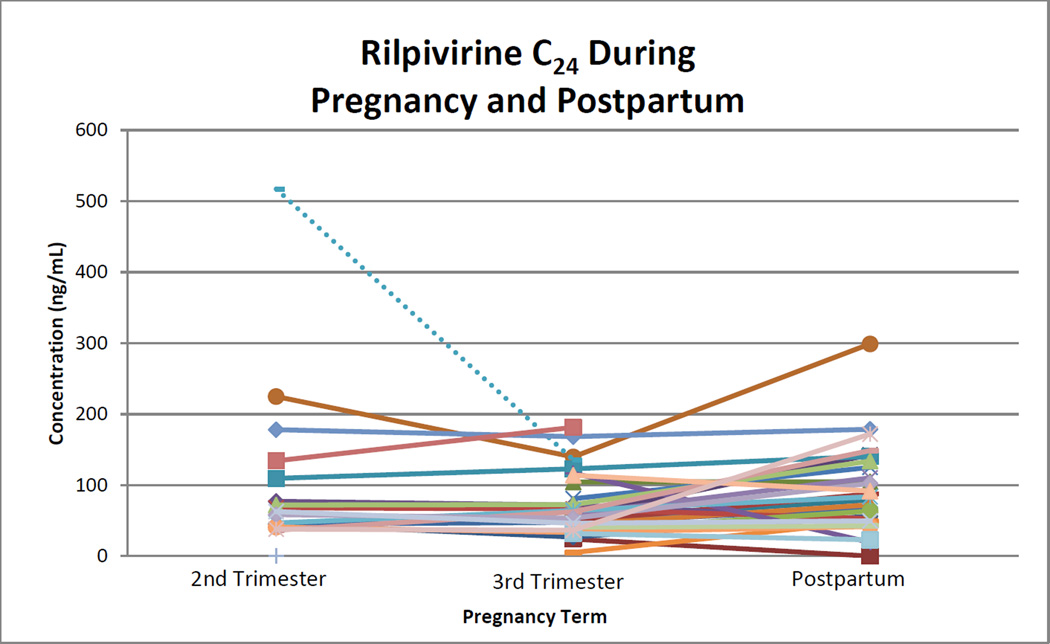
Results: Median (range) AUC0-24 were 1969 (867-4987, n = 15), 1669 (556-4312, n = 28), and 2387 (188-6736, n = 28) ng·h/mL in the second trimester, the third trimester, and postpartum, respectively (P < 0.05 for either trimester vs postpartum). Median (range) C24 were 63 (37-225, n = 17), 56 (<10-181, n = 30), and 81 (<10-299, n = 28) ng/mL (P < 0.05 for either trimester vs postpartum). High variability in pharmacokinetic parameters was observed between subjects. Median (range) cord blood/maternal concentration ratio was 0.55 (0.3-0.8, n = 21). Delivery HIV-1 RNA was ≤50 copies per milliliter in 70% and ≤400 copies per milliliter in 90% of women. Cmin were significantly lower at 15 visits with detectable HIV-1 RNA compared with 61 visits with undetectable HIV-1 RNA, 29 (<10-93) vs 63 (15-200) ng/mL (P = 0.0001). Cmin was below the protein binding-adjusted EC90 concentration (12.2 ng/mL) at 4 visits in 3 of 31 women (10%).
Conclusions: Rilpivirine exposure is lower during pregnancy compared with postpartum and highly variable. Ninety percent of women had minimum concentrations above the protein binding-adjusted EC90 for rilpivirine.
Conflict of interest statement
Conflicts of Interest: All other co-authors have no conflicts (A.H.T., B.M.B., A.S., J.W., E.V.C., S.K.B., R.K., K.R., K.G., T.R.C., N.C., E.S., D.E.S.).
Figures
Similar articles
-
Lowered Rilpivirine Exposure During the Third Trimester of Pregnancy in Human Immunodeficiency Virus Type 1-Infected Women.Clin Infect Dis. 2017 Oct 15;65(8):1335-1341. doi: 10.1093/cid/cix534. Clin Infect Dis. 2017. PMID: 28595298 Clinical Trial.
-
Pharmacokinetics of tenofovir during pregnancy and postpartum.HIV Med. 2015 Sep;16(8):502-11. doi: 10.1111/hiv.12252. Epub 2015 May 11. HIV Med. 2015. PMID: 25959631 Free PMC article.
-
Efavirenz pharmacokinetics during the third trimester of pregnancy and postpartum.J Acquir Immune Defic Syndr. 2012 Mar 1;59(3):245-52. doi: 10.1097/QAI.0b013e31823ff052. J Acquir Immune Defic Syndr. 2012. PMID: 22083071 Free PMC article. Clinical Trial.
-
Pharmacokinetic optimization of antiretroviral therapy in pregnancy.Clin Pharmacokinet. 2012 Oct 1;51(10):639-59. doi: 10.1007/s40262-012-0002-0. Clin Pharmacokinet. 2012. PMID: 23018528 Review.
-
Pharmacokinetics of antiretrovirals in pregnant women.Clin Pharmacokinet. 2004;43(15):1071-87. doi: 10.2165/00003088-200443150-00002. Clin Pharmacokinet. 2004. PMID: 15568888 Review.
Cited by
-
Pharmacokinetic Adaptations in Pregnancy: Implications for Optimizing Antiretroviral Therapy in HIV-Positive Women.Pharmaceutics. 2025 Jul 15;17(7):913. doi: 10.3390/pharmaceutics17070913. Pharmaceutics. 2025. PMID: 40733121 Free PMC article. Review.
-
Implications of Bariatric Surgery on the Pharmacokinetics of Antiretrovirals in People Living with HIV.Clin Pharmacokinet. 2022 May;61(5):619-635. doi: 10.1007/s40262-022-01120-7. Epub 2022 Apr 11. Clin Pharmacokinet. 2022. PMID: 35404470 Free PMC article. Review.
-
Pharmacokinetics and Drug-Drug Interactions of Long-Acting Intramuscular Cabotegravir and Rilpivirine.Clin Pharmacokinet. 2021 Jul;60(7):835-853. doi: 10.1007/s40262-021-01005-1. Epub 2021 Apr 8. Clin Pharmacokinet. 2021. PMID: 33830459 Free PMC article. Review.
-
The role of rilpivirine in Southern Africa.South Afr J HIV Med. 2019 May 29;20(1):825. doi: 10.4102/sajhivmed.v20i1.825. eCollection 2019. South Afr J HIV Med. 2019. PMID: 31205774 Free PMC article.
-
Drug-Drug Interactions with Antiretroviral Drugs in Pregnant Women Living with HIV: Are They Different from Non-Pregnant Individuals?Clin Pharmacokinet. 2020 Oct;59(10):1217-1236. doi: 10.1007/s40262-020-00914-x. Clin Pharmacokinet. 2020. PMID: 32696442 Free PMC article. Review.
References
-
- [Accessed January 5, 2016];Global Update on the Health Sector Response to HIV. 2014 Available at http://apps.who.int/iris/bitstream/10665/128494/1/9789241507585_eng.pdf?....
-
- Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. [Accessed April 3, 2014];Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf.
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. [Accessed April 9, 2014];Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. Available at http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
-
- Colbers A, Greupink R, Burger D. Pharmacological considerations on the use of antiretrovirals in pregnancy. Curr Opin Infect Dis. 2013;26:575–588. - PubMed
-
- Helldén A, Madadi P. Pregnancy and pharmacogenomics in the context of drug metabolism and response. Pharmacogenomics. 2013;14:1779–1791. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
