

Host and parasite genetics shape a link between Trypanosoma cruzi infection dynamics and chronic cardiomyopathy
- PMID: 26918803
- PMCID: PMC5031194
- DOI: 10.1111/cmi.12584
Host and parasite genetics shape a link between Trypanosoma cruzi infection dynamics and chronic cardiomyopathy
Abstract
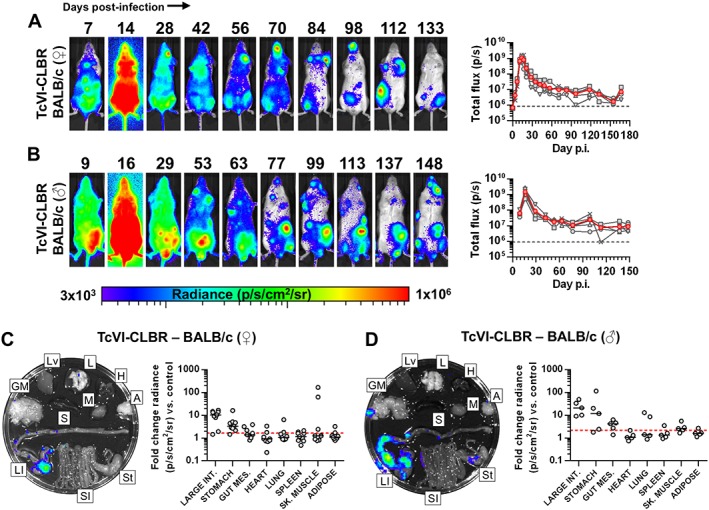
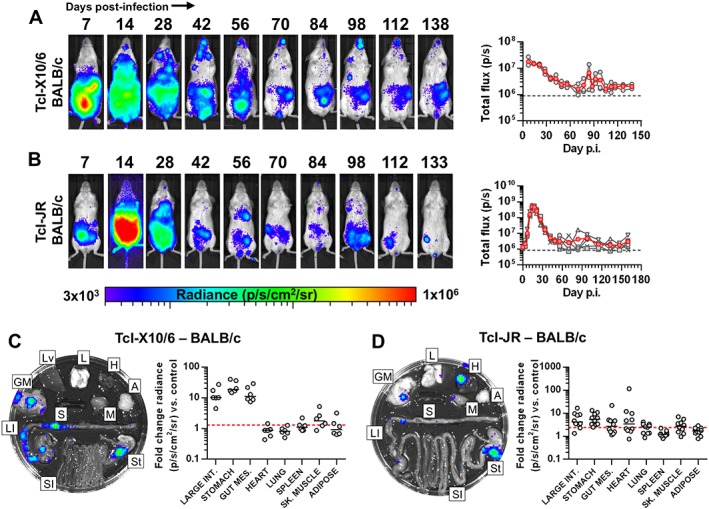
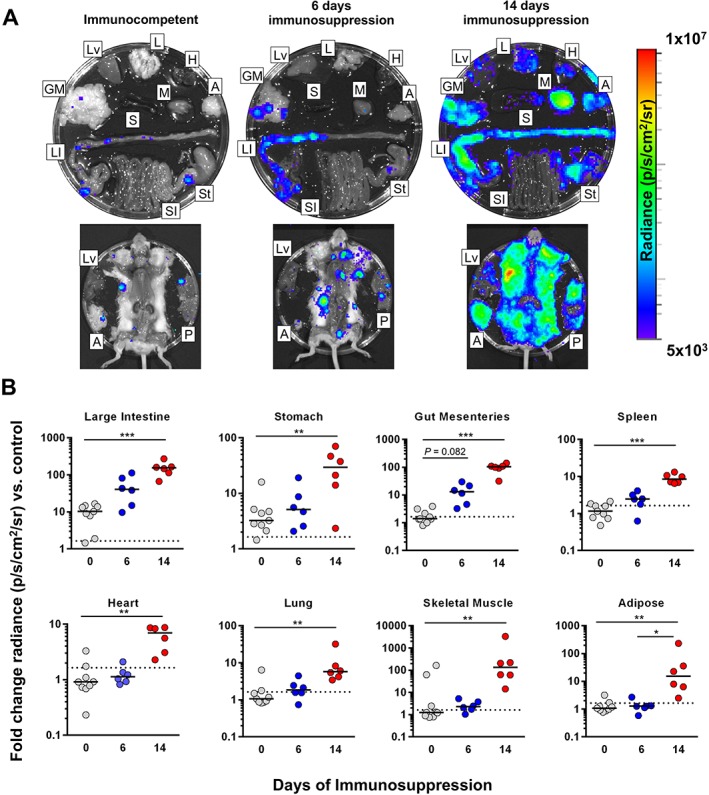
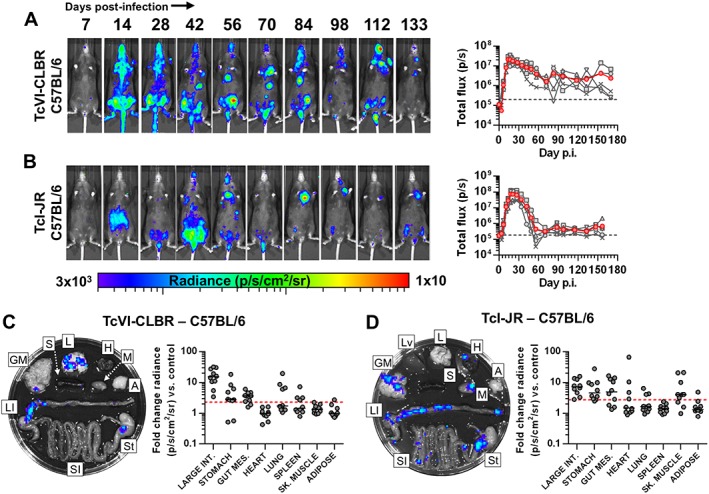
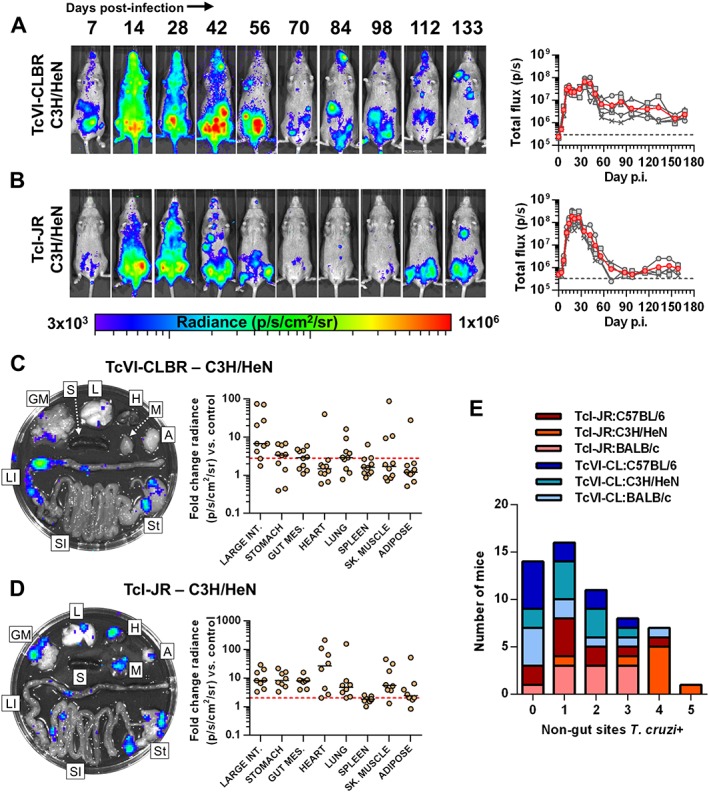
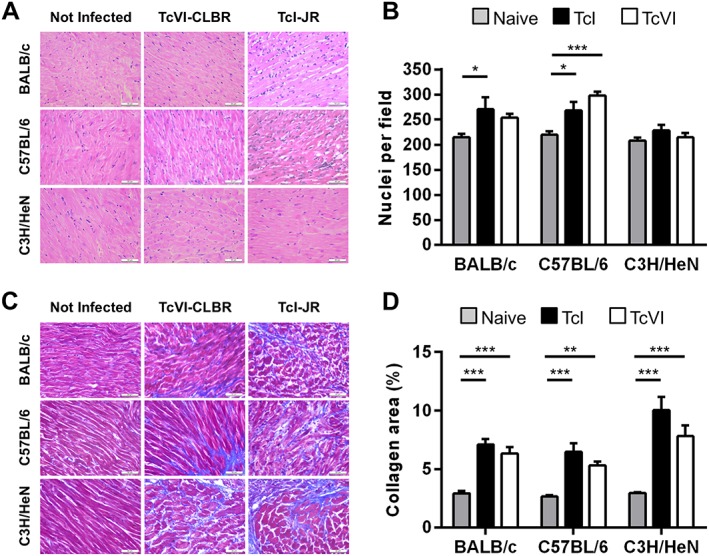
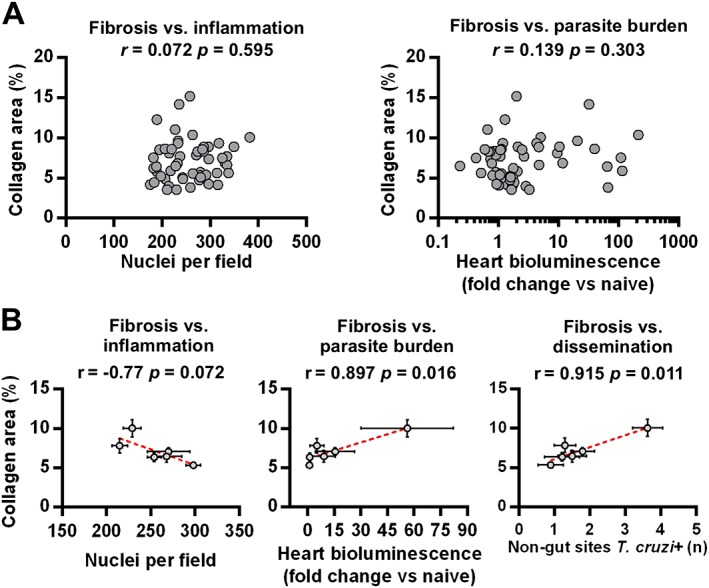
Host and parasite diversity are suspected to be key factors in Chagas disease pathogenesis. Experimental investigation of underlying mechanisms is hampered by a lack of tools to detect scarce, pleiotropic infection foci. We developed sensitive imaging models to track Trypanosoma cruzi infection dynamics and quantify tissue-specific parasite loads, with minimal sampling bias. We used this technology to investigate cardiomyopathy caused by highly divergent parasite strains in BALB/c, C3H/HeN and C57BL/6 mice. The gastrointestinal tract was unexpectedly found to be the primary site of chronic infection in all models. Immunosuppression induced expansion of parasite loads in the gut and was followed by widespread dissemination. These data indicate that differential immune control of T. cruzi occurs between tissues and shows that the large intestine and stomach provide permissive niches for active infection. The end-point frequency of heart-specific infections ranged from 0% in TcVI-CLBR-infected C57BL/6 to 88% in TcI-JR-infected C3H/HeN mice. Nevertheless, infection led to fibrotic cardiac pathology in all models. Heart disease severity was associated with the model-dependent frequency of dissemination outside the gut and inferred cumulative heart-specific parasite loads. We propose a model of cardiac pathogenesis driven by periodic trafficking of parasites into the heart, occurring at a frequency determined by host and parasite genetics.
© 2016 The Authors Cellular Microbiology Published by John Wiley & Sons Ltd.
Figures
References
-
- Adad, S.J. , Andrade, D.C.d.S. , Lopes, E.R. , and Chapadeiro, E. (1991) Contribuição ao estudo da anatomia patológica do megaesôfago chagásico. Rev I Med Trop 33: 443–450. - PubMed
-
- Albareda, M.C. , De Rissio, A.M. , Tomas, G. , Serjan, A. , Alvarez, M.G. , Viotti, R. , et al. (2013) Polyfunctional T cell responses in children in early stages of chronic Trypanosoma cruzi infection contrast with monofunctional responses of long‐term infected adults. PLoS Negl Trop Dis 7: e2575. - PMC - PubMed
-
- Andrade, S.G. (1990) Influence of Trypanosoma cruzi strain on the pathogenesis of chronic myocardiopathy in mice. Mem Inst Oswaldo Cruz 85: 17–27. - PubMed
-
- Añez, N. , Carrasco, H. , Parada, H. , Crisante, G. , Rojas, A. , Fuenmayor, C. , et al. (1999) Myocardial parasite persistence in chronic chagasic patients. Am J Trop Med Hyg 60: 726–732. - PubMed
-
- Bern, C. (2011) Antitrypanosomal therapy for chronic Chagas' disease. New Engl J Med 364: 2527–2534. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
