

Early Alterations in Glycemic Control and Pancreatic Endocrine Function in Nondiabetic Patients With Chronic Pancreatitis
- PMID: 26918872
- PMCID: PMC4783201
- DOI: 10.1097/MPA.0000000000000491
Early Alterations in Glycemic Control and Pancreatic Endocrine Function in Nondiabetic Patients With Chronic Pancreatitis
Abstract
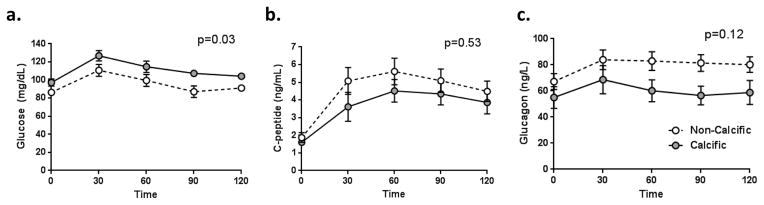
Objectives: Diabetes mellitus is a frequent consequence of chronic pancreatitis (CP). Little is known about pancreatic endocrine function before the development of diabetes mellitus in CP, particularly in females, or those without calcific and/or alcoholic pancreatitis.
Methods: Twenty-five nondiabetic adult patients with CP (19 female; mean [SE] age, 34.2 [2.4] years) were compared with 25 healthy controls matched for age, sex, and body mass index. Subjects underwent frequent sample intravenous glucose tolerance testing (FSIVGTT) and mixed meal tolerance testing (MMTT).
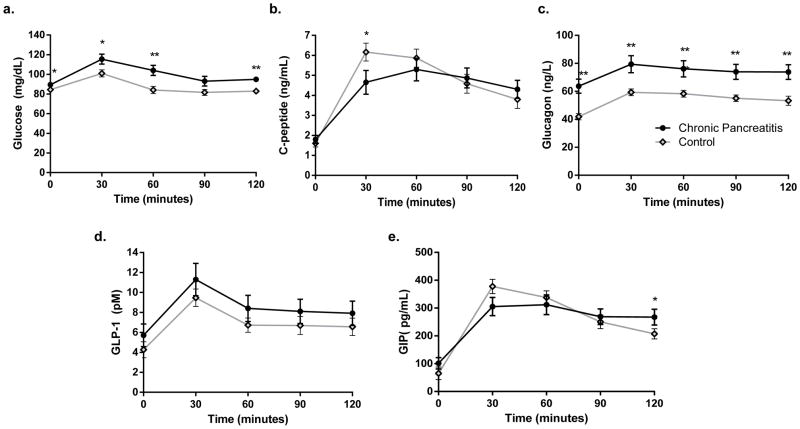
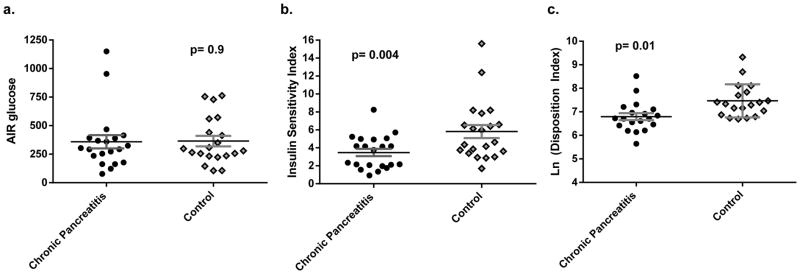
Results: Mean (SE) fasting glucose was higher in patients with CP (89.5 [2.3] mg/dL) than in controls (84.4 [1.2] mg/dL, P = 0.04). On MMTT, patients with CP had a higher area under the curve (AUC) glucose and AUC glucagon compared with controls (P ≤ 0.01). The AUC C-peptide was equivalent (P = 0.6) but stimulated C-peptide at 30 minutes was lower in patients with CP (P = 0.04). Mean insulin sensitivity index calculated from the FSIVGTT was lower in CP group, indicating reduced insulin sensitivity (P ≤ 0.01). Disposition index (insulin secretion adjusted for insulin sensitivity on FSIVGTT) was lower in patients with CP (P = 0.01).
Conclusions: Patients with CP had higher fasting and MMTT glucose levels, without a compensatory increase in insulin secretion suggesting subtle early islet dysfunction. Our cohort had relative hyperglucagonemia and was less insulin sensitive than controls.
Conflict of interest statement
Figures
References
-
- Ammann RW. Diagnosis and management of chronic pancreatitis: current knowledge. Swiss medical weekly: official journal of the Swiss Society of Infectious Diseases, the Swiss Society of Internal Medicine, the Swiss Society of Pneumology. 2006;136:166–74. - PubMed
-
- Braganza JM, Lee SH, McCloy RF, et al. Chronic pancreatitis. Lancet. 2011;377:1184–97. - PubMed
-
- Cui Y, Andersen DK. Pancreatogenic diabetes: special considerations for management. Pancreatology. 2011;11:279–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
