

The Efficacy of Multiparametric Magnetic Resonance Imaging and Magnetic Resonance Imaging Targeted Biopsy in Risk Classification for Patients with Prostate Cancer on Active Surveillance
- PMID: 26920465
- PMCID: PMC5540367
- DOI: 10.1016/j.juro.2016.02.084
The Efficacy of Multiparametric Magnetic Resonance Imaging and Magnetic Resonance Imaging Targeted Biopsy in Risk Classification for Patients with Prostate Cancer on Active Surveillance
Abstract
Purpose: We determined whether multiparametric magnetic resonance imaging targeted biopsies may replace systematic biopsies to detect higher grade prostate cancer (Gleason score 7 or greater) and whether biopsy may be avoided based on multiparametric magnetic resonance imaging among men with Gleason 3+3 prostate cancer on active surveillance.
Materials and methods: We identified men with previously diagnosed Gleason score 3+3 prostate cancer on active surveillance who underwent multiparametric magnetic resonance imaging and a followup prostate biopsy. Suspicion for higher grade cancer was scored on a standardized 5-point scale. All patients underwent a systematic biopsy. Patients with multiparametric magnetic resonance imaging regions of interest also underwent magnetic resonance imaging targeted biopsy. The detection rate of higher grade cancer was estimated for different multiparametric magnetic resonance imaging scores with the 3 biopsy strategies of systematic, magnetic resonance imaging targeted and combined.
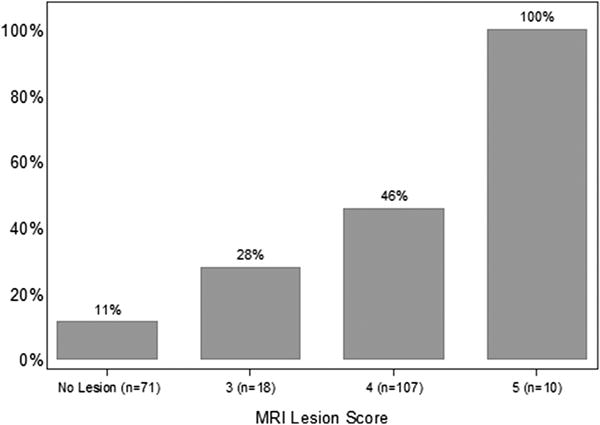
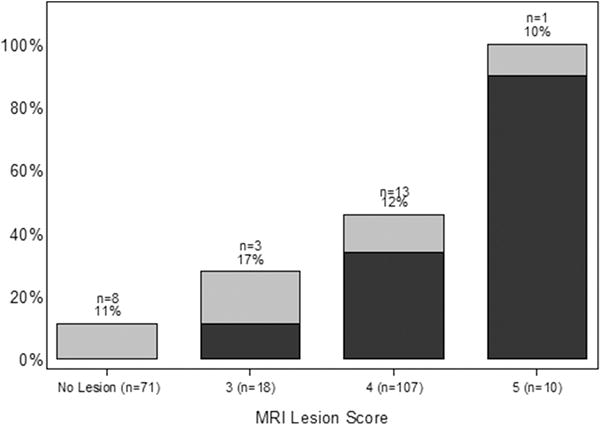
Results: Of 206 consecutive men on active surveillance 135 (66%) had a multiparametric magnetic resonance imaging region of interest. Overall, higher grade cancer was detected in 72 (35%) men. A higher multiparametric magnetic resonance imaging score was associated with an increased probability of detecting higher grade cancer (Wilcoxon-type trend test p <0.0001). Magnetic resonance imaging targeted biopsy detected higher grade cancer in 23% of men. Magnetic resonance imaging targeted biopsy alone missed higher grade cancers in 17%, 12% and 10% of patients with multiparametric magnetic resonance imaging scores of 3, 4 and 5, respectively.
Conclusions: Magnetic resonance imaging targeted biopsies increased the detection of higher grade cancer among men on active surveillance compared to systematic biopsy alone. However, a clinically relevant proportion of higher grade cancer was detected using only systematic biopsy. Despite the improved detection of disease progression using magnetic resonance imaging targeted biopsy, systematic biopsy cannot be excluded as part of surveillance for men with low risk prostate cancer.
Keywords: image-guided biopsy; magnetic resonance imaging; prostatic neoplasms; watchful waiting.
Copyright © 2016 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Editorial Comment.J Urol. 2016 Aug;196(2):381. doi: 10.1016/j.juro.2016.02.2991. Epub 2016 May 4. J Urol. 2016. PMID: 27154560 Free PMC article. No abstract available.
-
Editorial Comment.J Urol. 2016 Aug;196(2):380-1. doi: 10.1016/j.juro.2016.02.2990. Epub 2016 May 4. J Urol. 2016. PMID: 27154561 No abstract available.
References
-
- Mohler J, Armstrong AJ, Bahnson RR, et al. Prostate cancer, Version 3.2012: featured updates to the NCCN guidelines. J Natl Compr Canc Netw. 2012;10:1081–7. - PubMed
-
- Conti SL, Dall’era M, Fradet V, Cowan JE, Simko J, Carroll PR. Pathological outcomes of candidates for active surveillance of prostate cancer. J Urol. 2009;181:1628–33. - PubMed
-
- Lee MC, Dong F, Stephenson AJ, Jones JS, Magi-Galluzzi C, Klein EA. The Epstein criteria predict for organ-confined but not insignificant disease and a high likelihood of cure at radical prostatectomy. Eur Urol. 2010;58:90–5. - PubMed
-
- Klotz L, Vesprini D, Sethukavalan P, et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol. 2015;33:272–7. - PubMed
-
- Pokorny MR, de Rooij M, Duncan E, et al. Prospective study of diagnostic accuracy comparing prostate cancer detection by transrectal ultrasound-guided biopsy versus magnetic resonance (MR) imaging with subsequent MR-guided biopsy in men without previous prostate biopsies. Eur Urol. 2014;66:22–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
