

Effect of Contemporary Bariatric Surgical Procedures on Type 2 Diabetes Remission. A Population-Based Matched Cohort Study
- PMID: 26922184
- PMCID: PMC5018032
- DOI: 10.1007/s11695-016-2103-6
Effect of Contemporary Bariatric Surgical Procedures on Type 2 Diabetes Remission. A Population-Based Matched Cohort Study
Abstract
Objective: The objective of the study is to evaluate the effect of gastric banding, gastric bypass and sleeve gastrectomy on medium to long-term diabetes control in obese participants with type 2 diabetes mellitus.
Research design and methods: Matched cohort study using primary care electronic health records from the UK Clinical Practice Research Datalink. Obese participants with type 2 diabetes who received bariatric surgery from 2002 to 2014 were compared with matched control participants who did not receive BS. Remission was defined for each year of follow-up as HbA1c <6.5 % and no antidiabetic drugs prescribed.
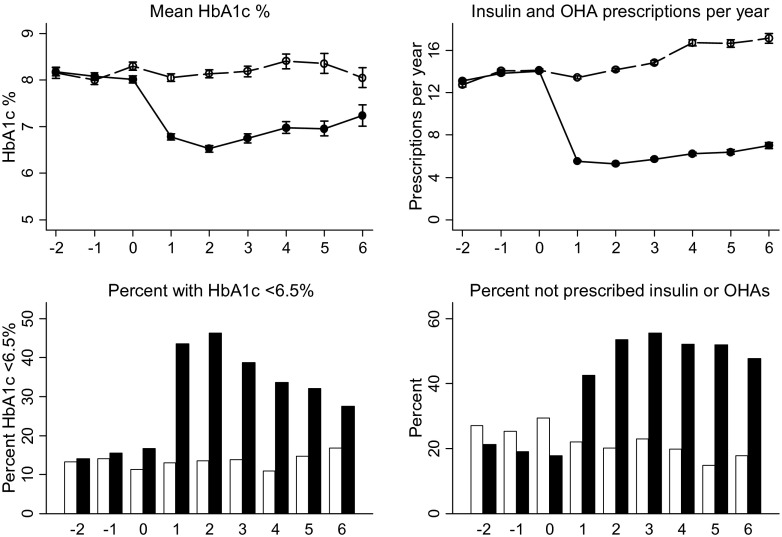
Results: There were 826 obese participants with T2DM who received bariatric surgery including adjustable gastric banding (LAGB) 220; gastric bypass (GBP) 449; or sleeve gastrectomy (SG) 153; with four procedures undefined. Mean HbA1c declined from 8.0 % before BS to 6.5 % in the second postoperative year; proportion with HbA1c <6.5 % (<48 mmol/mol) increased from 17 to 47 %. The proportion of patients in remission was 30 % in the second year, being 20 % for LAGB, 34 % for GBP and 38 % for SG. The adjusted relative rate of remission over the first six postoperative years was 5.97 (4.86 to 7.33, P < 0.001) overall; for LAGB 3.32 (2.27 to 4.86); GBP 7.16 (5.64 to 9.08); and SG 6.82 (5.05 to 9.19). Rates of remission were maintained into the sixth year of follow-up.
Conclusions: Remission of diabetes may continue for up to 6 years after bariatric surgical procedures. Diabetes outcomes are generally more favourable after gastric bypass or sleeve gastrectomy than LAGB.
Keywords: Antidiabetes drugs; Bariatric surgery; Electronic health records; Primary care; Type 2 diabetes mellitus.
Conflict of interest statement
Compliance with Ethical Standards Collaborators The King’s Bariatric Surgery Study Group also includes Mark Ashworth, Alex Dregan, Peter Littlejohns and Caroline Rudisill. Funding This research was supported by the UK National Institutes for Health Research (NIHR) Health Services and Delivery Research programme (12/5005/12). The funders did not engage in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. Martin Gulliford and Toby Prevost are supported by the NIHR Biomedical Research Centre at Guy’s and St Thomas’ National Health Service Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the National Health Service, the National Institute of Health Research or the Department of Health. This study is based in part on data from the Clinical Practice Research Datalink obtained under licence from the UK Medicines and Healthcare products Regulatory Agency. However, the interpretation and conclusions contained in this report are those of the authors alone. Conflict of Interest None to declare. Ethical Approval For this type of study, formal consent is not required. Informed Consent Does not apply. Contribution Statement MG and HB contributed to the conceptualisation, design, acquisition, analysis and interpretation of data, and writing of the manuscript. OK contributed to the interpretation of data and critical revision of the manuscript for important intellectual content. JC contributed to the analysis and interpretation of data and critical revision of the manuscript. AF contributed to the interpretation of data, the writing of the manuscript and critical revision of the manuscript. MR and ATP contributed to the design, interpretation of data and to the critical revision of the manuscript for important intellectual content. All authors gave final approval of the version to be published. MG is the guarantor of this work.
Figures
References
-
- Booth H, Khan O, Prevost T, Reddy M, Dregan A, Charlton J, et al. Incidence of type 2 diabetes after bariatric surgery: population-based matched cohort study. The Lancet Diab Endocrinol. 2014. - PubMed
-
- National Institute for Health and Care Excellence . Obesity: identification, assessment and management of overweight and obesity in children, young people and adults (draft for consultation) London: National Institute for Health and Care Excellence; 2014. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
