

Neurointerventional management of carotid webs associated with recurrent and acute cerebral ischemic syndromes
- PMID: 26922976
- PMCID: PMC4984381
- DOI: 10.1177/1591019916633245
Neurointerventional management of carotid webs associated with recurrent and acute cerebral ischemic syndromes
Abstract
Background: A carotid web can be defined as an endoluminal shelf-like projection often noted at the origin of the internal carotid artery (ICA) just beyond the bifurcation. Diagnosis of a carotid web as an underlying cause of recurrent ischemic stroke is infrequent and easily misdiagnosed as an atheromatous plaque. Surgery has traditionally been used to resect symptomatic lesions while there is no enough evidence supporting medical therapy as the sole management. To our knowledge there is only one report about carotid artery stenting (CAS) as a definite management of carotid web and no previous reports of acute large-vessel occlusions undergoing mechanical thrombectomy in the setting of carotid web as the etiology.
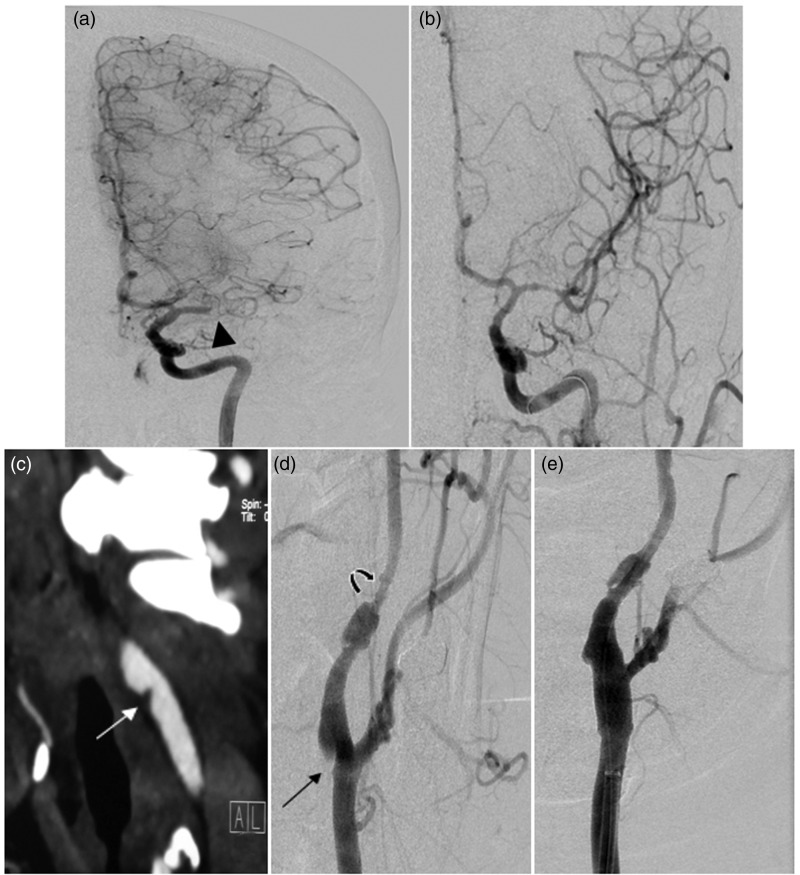
Case report: We report two cases: The first presented with recurrent ischemic stroke in the same arterial territory and the other with an emergent left middle cerebral artery (MCA) occlusion that underwent endovascular mechanical thrombectomy in which initial computed tomographic angiograms (CTA) suggested carotid web etiologies. Following confirmation with digital subtraction angiography (DSA), both patients ultimately underwent endovascular carotid stenting instead of surgical resection for definitive carotid web treatment.
Conclusions: Carotid webs are a rare cause of ischemic stroke in young and middle-aged adults that can readily be identified by CTA. Endovascular management may include emergent mechanical thrombectomy for large-vessel thromboembolic complications, and for definitive treatment with carotid stenting across the carotid web as an alternative to surgical resection and medical management for secondary stroke prevention.
Keywords: Carotid; recurrent; stent; stroke; web.
© The Author(s) 2016.
Figures

References
-
- Ehrenfeld WK, Stoney RJ, Wylie EJ. Fibromuscular hyperplasia of the internal carotid artery. Arch Surg 1967; 95: 284–287. - PubMed
-
- Houser OW, Baker HL, Jr, Sandok BA, et al. Cephalic arterial fibromuscular dysplasia. Radiology 1971; 101: 605–611. - PubMed
-
- Joux J, Chausson N, Jeannin S, et al. Carotid-bulb atypical fibromuscular dysplasia in young Afro-Caribbean patients with stroke. Stroke 2014; 45: 3711–3713. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
