

Dual-pathway multi-echo sequence for simultaneous frequency and T2 mapping
- PMID: 26923150
- PMCID: PMC4818735
- DOI: 10.1016/j.jmr.2016.01.019
Dual-pathway multi-echo sequence for simultaneous frequency and T2 mapping
Abstract
Purpose: To present a dual-pathway multi-echo steady state sequence and reconstruction algorithm to capture T2, T2(∗) and field map information.
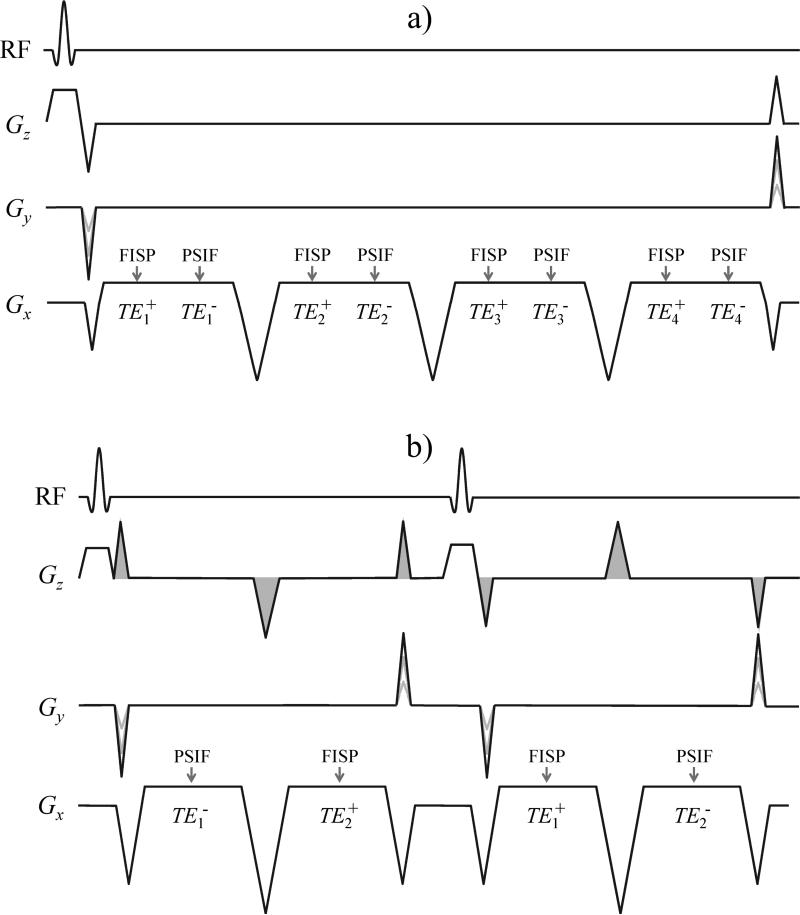
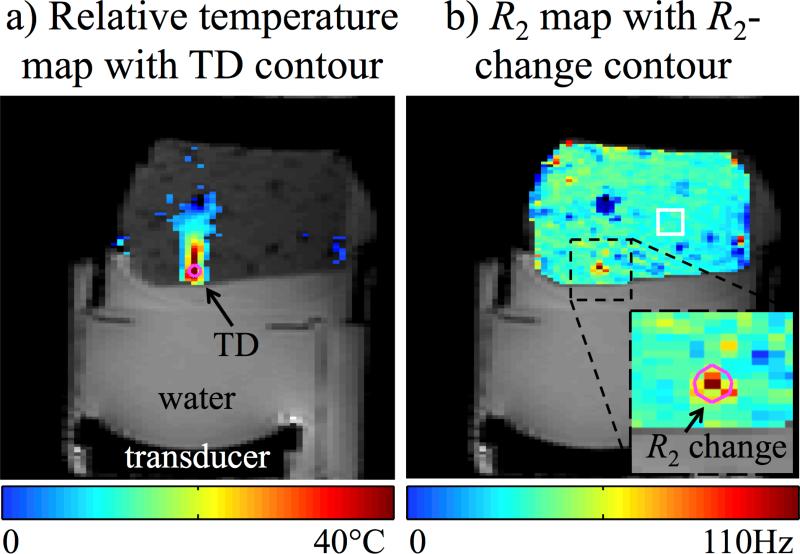
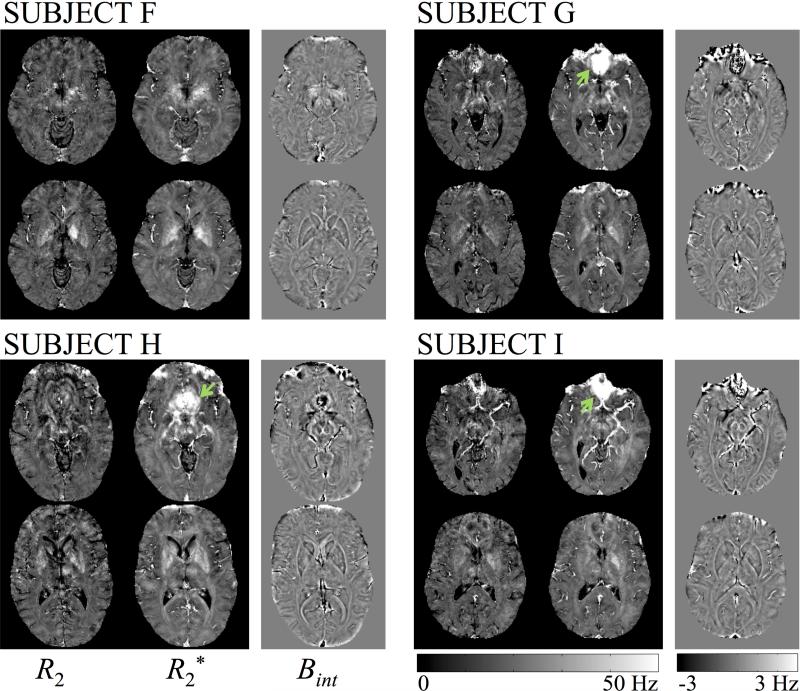
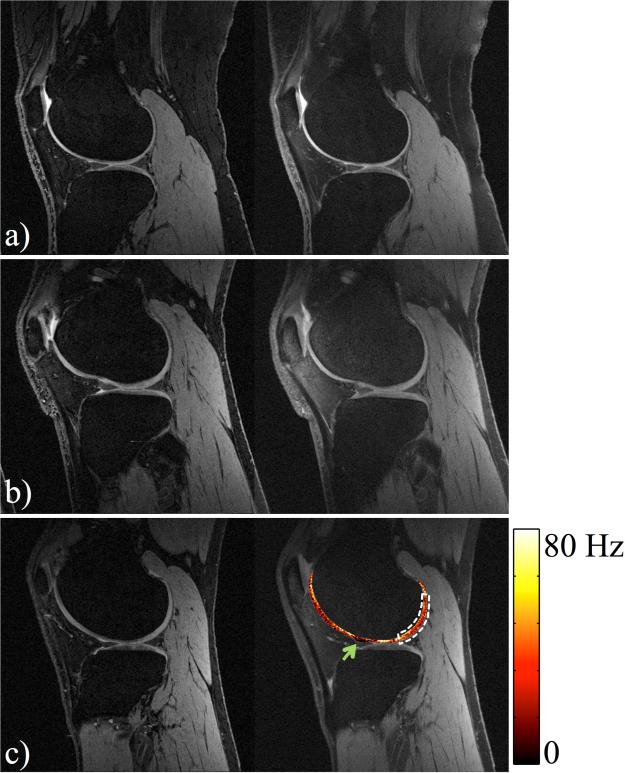
Methods: Typically, pulse sequences based on spin echoes are needed for T2 mapping while gradient echoes are needed for field mapping, making it difficult to jointly acquire both types of information. A dual-pathway multi-echo pulse sequence is employed here to generate T2 and field maps from the same acquired data. The approach might be used, for example, to obtain both thermometry and tissue damage information during thermal therapies, or susceptibility and T2 information from a same head scan, or to generate bonus T2 maps during a knee scan.
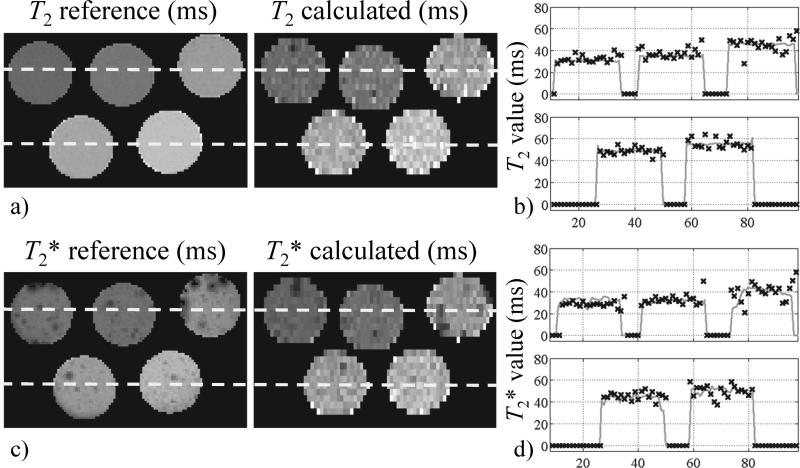
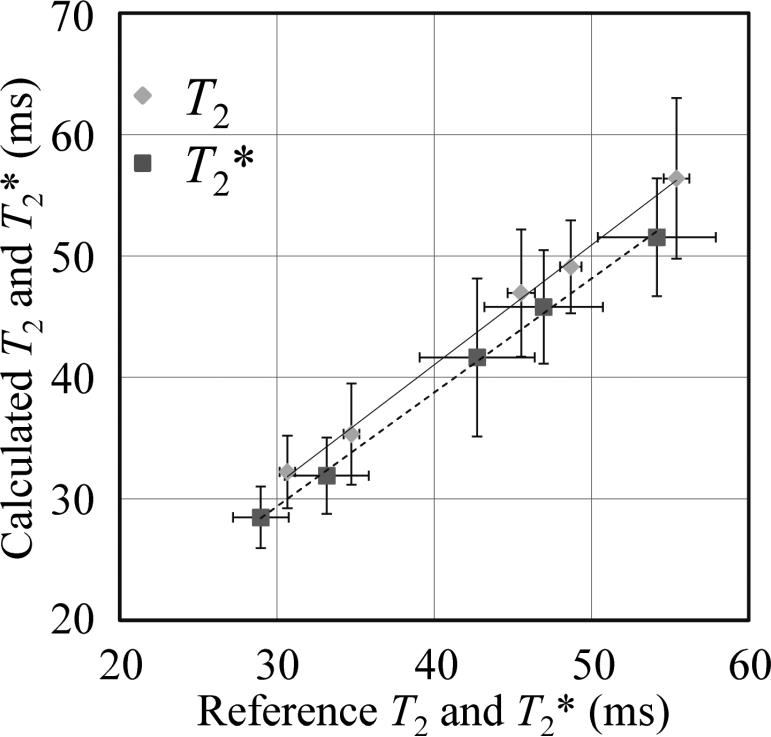
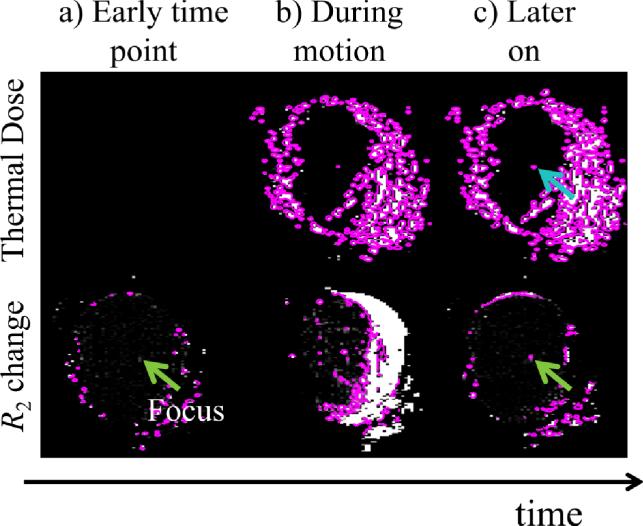
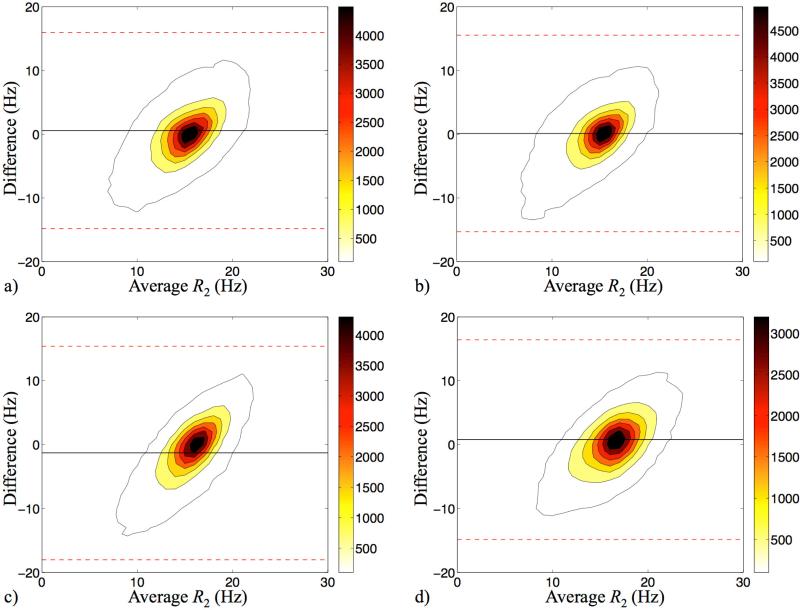
Results: Quantitative T2, T2(∗) and field maps were generated in gel phantoms, ex vivo bovine muscle, and twelve volunteers. T2 results were validated against a spin-echo reference standard: A linear regression based on ROI analysis in phantoms provided close agreement (slope/R(2)=0.99/0.998). A pixel-wise in vivo Bland-Altman analysis of R2=1/T2 showed a bias of 0.034 Hz (about 0.3%), as averaged over four volunteers. Ex vivo results, with and without motion, suggested that tissue damage detection based on T2 rather than temperature-dose measurements might prove more robust to motion.
Conclusion: T2, T2(∗) and field maps were obtained simultaneously, from the same datasets, in thermometry, susceptibility-weighted imaging and knee-imaging contexts.
Keywords: Field mapping; MR thermometry; Multi-pathway imaging; Osteoarthritis; Quantitative imaging; Susceptibility-weighted imaging; T(2) mapping.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Haacke EM, Xu Y, Cheng YC, Reichenbach JR. Susceptibility weighted imaging (SWI). Magn Reson Med. 2004;52(3):612–618. - PubMed
-
- Haacke EM, Cheng NY, House MJ, Liu Q, Neelavalli J, Ogg RJ, Khan A, Ayaz M, Kirsch W, Obenaus A. Imaging iron stores in the brain using magnetic resonance imaging. Magn Reson Imaging. 2005;23(1):1–25. - PubMed
-
- Langkammer C, Krebs N, Goessler W, Scheurer E, Ebner F, Yen K, Fazekas F, Ropele S. Quantitative MR imaging of brain iron: a postmortem validation study. Radiology. 2010;257(2):455–462. - PubMed
-
- De Poorter J, De Wagter C, De Deene Y, Thomsen C, Stahlberg F, Achten E. Noninvasive MRI thermometry with the proton resonance frequency (PRF) method: in vivo results in human muscle. Magn Reson Med. 1995;33(1):74–81. - PubMed
-
- Ishihara Y, Calderon A, Watanabe H, Okamoto K, Suzuki Y, Kuroda K. A precise and fast temperature mapping using water proton chemical shift. Magn Reson Med. 1995;34(6):814–823. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
