

Challenges and opportunities for stem cell therapy in patients with chronic kidney disease
- PMID: 26924058
- PMCID: PMC4801657
- DOI: 10.1016/j.kint.2015.11.023
Challenges and opportunities for stem cell therapy in patients with chronic kidney disease
Abstract
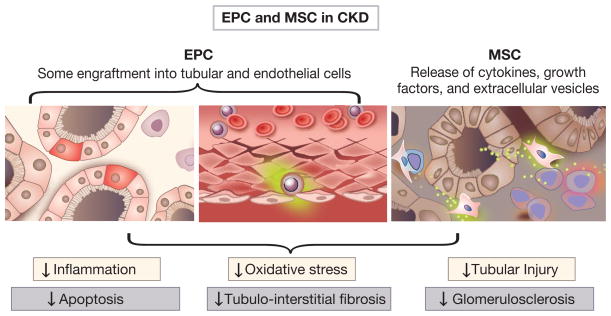
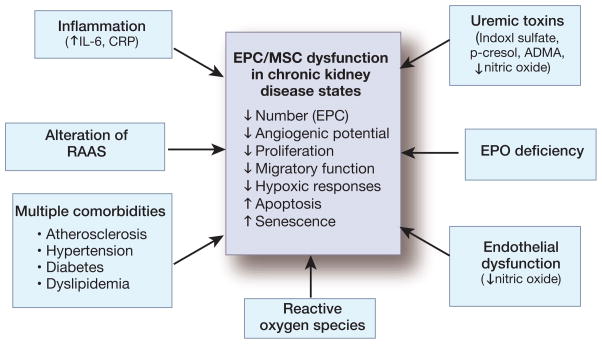
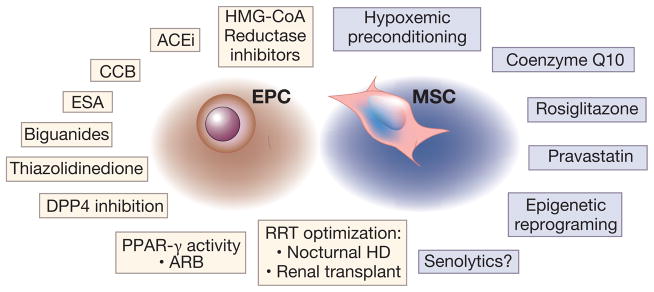
Chronic kidney disease (CKD) is a global health care burden affecting billions of individuals worldwide. The kidney has limited regenerative capacity from chronic insults, and for the most common causes of CKD, no effective treatment exists to prevent progression to end-stage kidney failure. Therefore, novel interventions, such as regenerative cell-based therapies, need to be developed for CKD. Given the risk of allosensitization, autologous transplantation of cells to boost regenerative potential is preferred. Therefore, verification of cell function and vitality in CKD patients is imperative. Two cell types have been most commonly applied in regenerative medicine. Endothelial progenitor cells contribute to neovasculogenesis primarily through paracrine angiogenic activity and partly by differentiation into mature endothelial cells in situ. Mesenchymal stem cells also exert paracrine effects, including proangiogenic, anti-inflammatory, and antifibrotic activity. However, in CKD, multiple factors may contribute to reduced cell function, including older age, coexisting cardiovascular disease, diabetes, chronic inflammatory states, and uremia, which may limit the effectiveness of an autologous cell-based therapy approach. This Review highlights current knowledge on stem and progenitor cell function and vitality, aspects of the uremic milieu that may serve as a barrier to therapy, and novel methods to improve stem cell function for potential transplantation.
Keywords: end-stage renal disease; senescence; stem cells; uremia.
Copyright © 2016 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382:260–272. - PubMed
-
- USRDS USRDS. Annual Data Report. Vol. 2015. Bethesda: 2014. Chapter 1: CKD in the General Population. 2014 Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. p Chronic Kidney Disease chapter.
-
- Hickson LJ, Cosio FG, El-Zoghby ZM, et al. Survival of patients on the kidney transplant wait list: relationship to cardiac troponin T. Am J Transplant. 2008;8:2352–2359. - PubMed
-
- Hickson LJ, El-Zoghby ZM, Lorenz EC, et al. Patient survival after kidney transplantation: relationship to pretransplant cardiac troponin T levels. Am J Transplant. 2009;9:1354–1361. - PubMed
-
- Schoonover KL, Hickson LJ, Norby SM, et al. Risk factors for hospitalization among older, incident haemodialysis patients. Nephrology (Carlton) 2013;18:712–717. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
