

Pathogenesis of Staphylococcus aureus Bloodstream Infections
- PMID: 26925499
- PMCID: PMC5068359
- DOI: 10.1146/annurev-pathol-012615-044351
Pathogenesis of Staphylococcus aureus Bloodstream Infections
Abstract
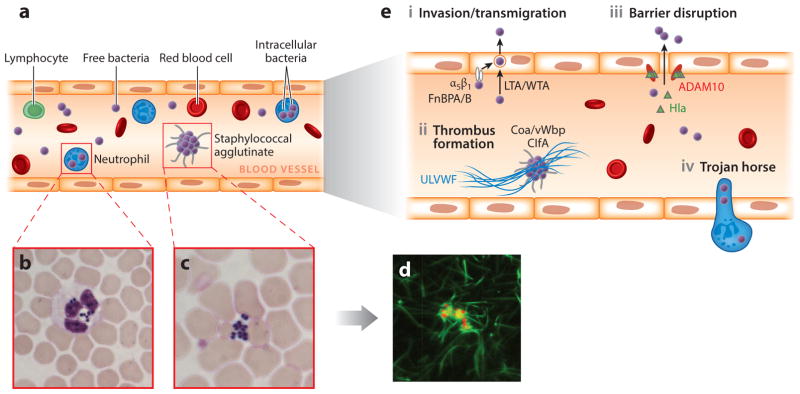
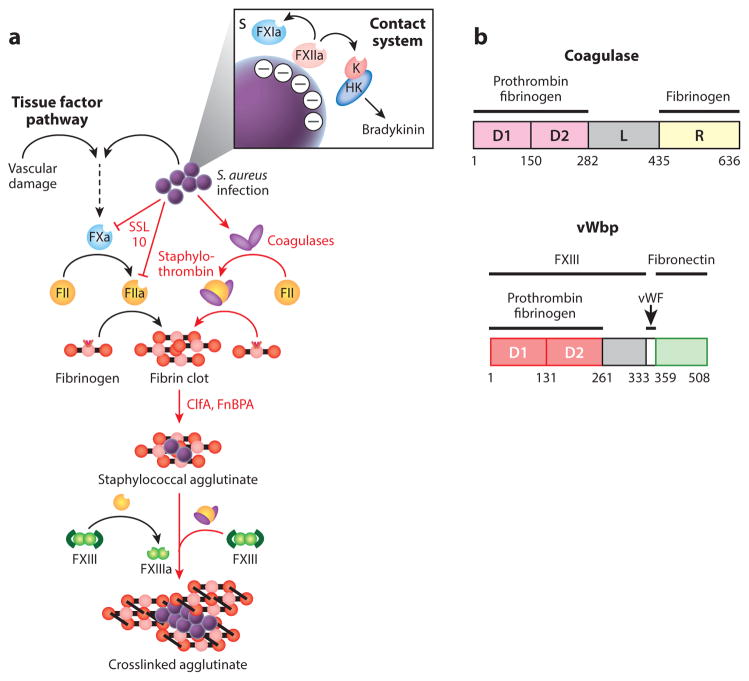
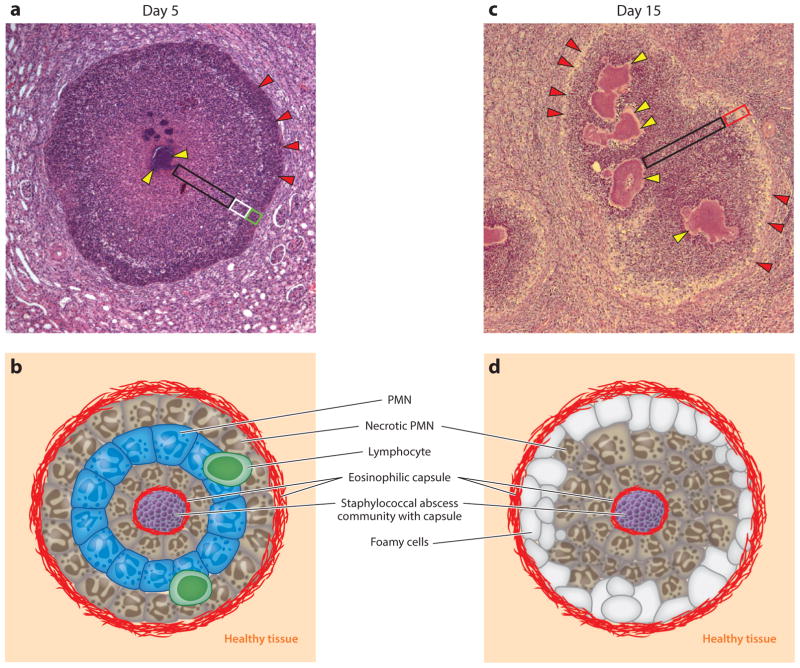
Staphylococcus aureus, a Gram-positive bacterium colonizing nares, skin, and the gastrointestinal tract, frequently invades the skin, soft tissues, and bloodstreams of humans. Even with surgical and antibiotic therapy, bloodstream infections are associated with significant mortality. The secretion of coagulases, proteins that associate with and activate the host hemostatic factor prothrombin, and the bacterial surface display of agglutinins, proteins that bind polymerized fibrin, are key virulence strategies for the pathogenesis of S. aureus bloodstream infections, which culminate in the establishment of abscess lesions. Pathogen-controlled processes, involving a wide spectrum of secreted factors, are responsible for the recruitment and destruction of immune cells, transforming abscess lesions into purulent exudate, with which staphylococci disseminate to produce new infectious lesions or to infect new hosts. Research on S. aureus bloodstream infections is a frontier for the characterization of protective vaccine antigens and the development of immune therapeutics aiming to prevent disease or improve outcomes.
Keywords: abscess formation; agglutination; coagulation; immune evasion; vaccine.
Figures
References
-
- van Belkum A, Melles DC, Nouwen J, van Leeuwen WB, van Wamel W, et al. Co-evolutionary aspects of human colonisation and infection by Staphylococcus aureus. Infect Genet Evol. 2009;9:32–47. - PubMed
-
- Liu C, Bayer AS, Cosgrove SE, Daum RS, Fridkin SK, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52:285–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
