

Easily identified at-risk patients for extubation failure may benefit from noninvasive ventilation: a prospective before-after study
- PMID: 26926168
- PMCID: PMC4770688
- DOI: 10.1186/s13054-016-1228-2
Easily identified at-risk patients for extubation failure may benefit from noninvasive ventilation: a prospective before-after study
Abstract
Background: While studies have suggested that prophylactic noninvasive ventilation (NIV) could prevent post-extubation respiratory failure in the intensive care unit, they appear inconsistent with regard to reintubation. We assessed the impact of a prophylactic NIV protocol on reintubation in a large population of at-risk patients.
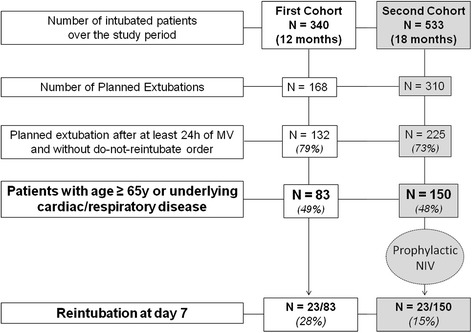
Methods: Prospective before-after study performed in the medical ICU of a teaching referral hospital. In the control cohort, we determined that patients older than 65 years and those with underlying cardiac or respiratory disease were at high-risk for reintubation. In the interventional cohort, we implemented a protocol using prophylactic NIV in all patients intubated at least 24 h and having one of these risk factors. NIV was immediately applied after planned extubation during at least the first 24 hours. Extubation failure was defined by the need for reintubation within seven days following extubation.
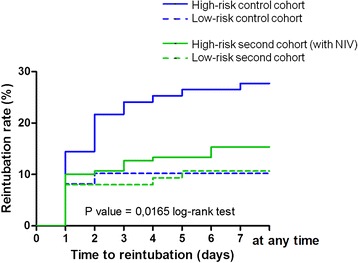
Results: We included 83 patients at high-risk among 132 extubated patients in the control cohort (12-month period) and 150 patients at high-risk among 225 extubated patients in the NIV cohort (18-month period). The reintubation rate was significantly decreased from 28% in the control cohort (23/83) to 15% (23/150) in the NIV cohort (p = 0.02 log-rank test), whereas the non-at-risk patients did not significantly differ in the two periods (10.2% vs. 10.7%, p = 0.93). After multivariate logistic-regression analysis, the use of prophylactic NIV protocol was independently associated with extubation success.
Conclusions: The implementation of prophylactic NIV after extubation may reduce the reintubation rate in a large population of patients with easily identified risk factors for extubation failure.
Figures
Comment in
-
Using noninvasive ventilation to prevent extubation failure: it is good news, but do we really know what "high risk" means?Crit Care. 2016 Jul 4;20(1):213. doi: 10.1186/s13054-016-1336-z. Crit Care. 2016. PMID: 27389025 Free PMC article. No abstract available.
References
-
- Thille AW, Harrois A, Schortgen F, Brun-Buisson C, Brochard L. Outcomes of extubation failure in medical intensive care unit patients. Crit Care Med. 2011;39(12):2612–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
