

Urinary Glycosaminoglycans Predict Outcomes in Septic Shock and Acute Respiratory Distress Syndrome
- PMID: 26926297
- PMCID: PMC5003330
- DOI: 10.1164/rccm.201511-2281OC
Urinary Glycosaminoglycans Predict Outcomes in Septic Shock and Acute Respiratory Distress Syndrome
Abstract
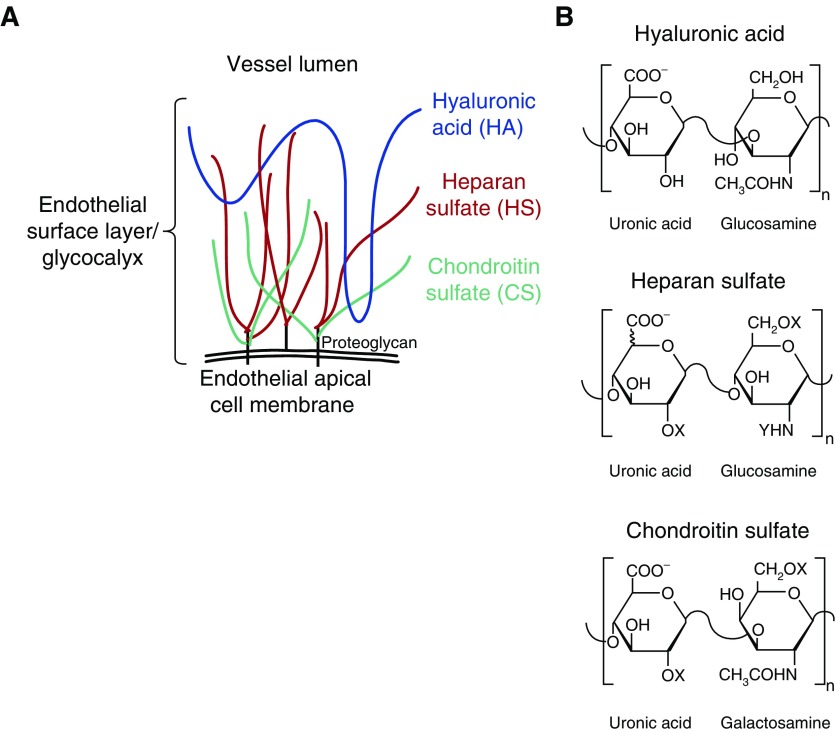
Rationale: Degradation of the endothelial glycocalyx, a glycosaminoglycan (GAG)-rich layer lining the vascular lumen, is associated with the onset of kidney injury in animal models of critical illness. It is unclear if similar pathogenic degradation occurs in critically ill patients.
Objectives: To determine if urinary indices of GAG fragmentation are associated with outcomes in patients with critical illnesses such as septic shock or acute respiratory distress syndrome (ARDS).
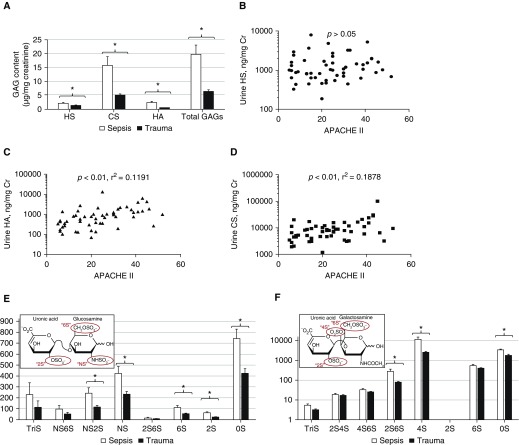
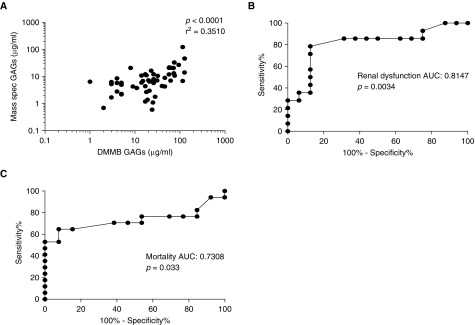
Methods: We prospectively collected urine from 30 patients within 24 hours of admission to the Denver Health Medical Intensive Care Unit (ICU) for septic shock. As a nonseptic ICU control, we collected urine from 25 surgical ICU patients admitted for trauma. As a medical ICU validation cohort, we obtained serially collected urine samples from 70 patients with ARDS. We performed mass spectrometry on urine samples to determine GAG (heparan sulfate, chondroitin sulfate, and hyaluronic acid) concentrations as well as patterns of heparan sulfate/chondroitin sulfate disaccharide sulfation. We compared these indices to measurements obtained using dimethylmethylene blue, an inexpensive, colorimetric urinary assay of sulfated GAGs.
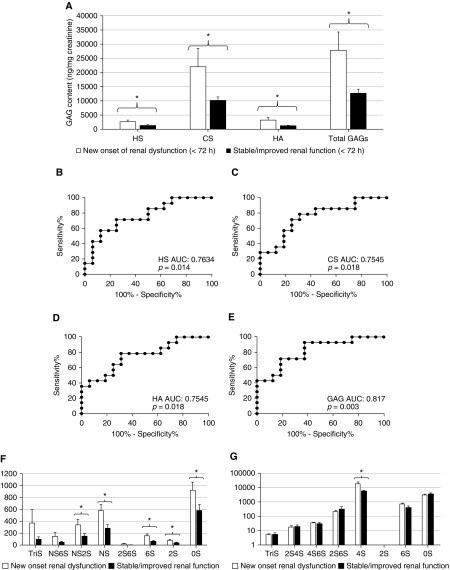
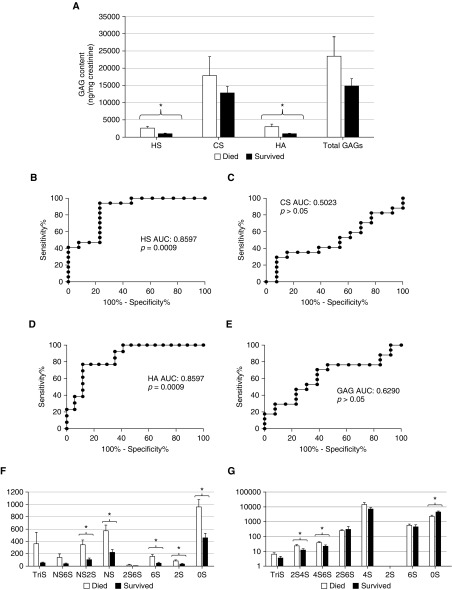
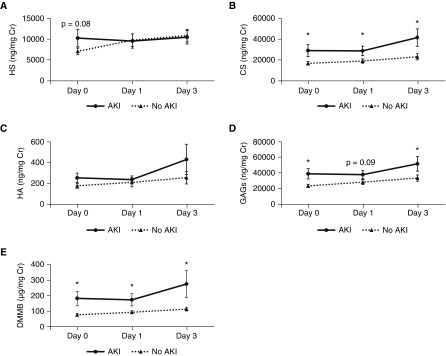
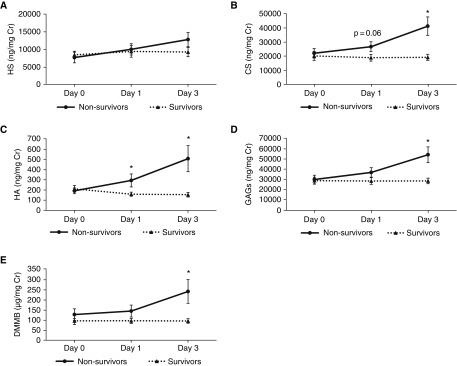
Measurements and main results: In septic shock, indices of GAG fragmentation correlated with both the development of renal dysfunction over the 72 hours after urine collection and with hospital mortality. This association remained after controlling for severity of illness and was similarly observed using the inexpensive dimethylmethylene blue assay. These predictive findings were corroborated using urine samples previously collected at three consecutive time points from patients with ARDS.
Conclusions: Early indices of urinary GAG fragmentation predict acute kidney injury and in-hospital mortality in patients with septic shock or ARDS. Clinical trial registered with www.clinicaltrials.gov (NCT01900275).
Keywords: chondroitin sulfate; glycocalyx; glycomics; heparan sulfate; hyaluronic acid.
Figures
Comment in
-
Endothelial Glycocalyx: Not Just a Sugar Coat.Am J Respir Crit Care Med. 2016 Aug 15;194(4):390-3. doi: 10.1164/rccm.201603-0624ED. Am J Respir Crit Care Med. 2016. PMID: 27525457 Free PMC article. No abstract available.
References
-
- Baron RM, Baron MJ, Perrella MA. Pathobiology of sepsis: are we still asking the same questions? Am J Respir Cell Mol Biol. 2006;34:129–134. - PubMed
-
- Liu V, Escobar GJ, Greene JD, Soule J, Whippy A, Angus DC, Iwashyna TJ. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312:90–92. - PubMed
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, et al. EPIC II Group of Investigators. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302:2323–2329. - PubMed
-
- Vincent J-L, Marshall JC, Ñamendys-Silva SA, François B, Martin-Loeches I, Lipman J, Reinhart K, Antonelli M, Pickkers P, Njimi H, et al. ICON investigators. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014;2:380–386. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
