

Detection of Occult Micrometastases in Patients With Clinical Stage I Non-Small-Cell Lung Cancer: A Prospective Analysis of Mature Results of CALGB 9761 (Alliance)
- PMID: 26926677
- PMCID: PMC4872306
- DOI: 10.1200/JCO.2015.63.4543
Detection of Occult Micrometastases in Patients With Clinical Stage I Non-Small-Cell Lung Cancer: A Prospective Analysis of Mature Results of CALGB 9761 (Alliance)
Abstract
Purpose: Outcomes after resection of stage I non-small-cell lung cancer (NSCLC) are variable, potentially due to undetected occult micrometastases (OM). Cancer and Leukemia Group B 9761 was a prospectively designed study aimed at determining the prognostic significance of OM.
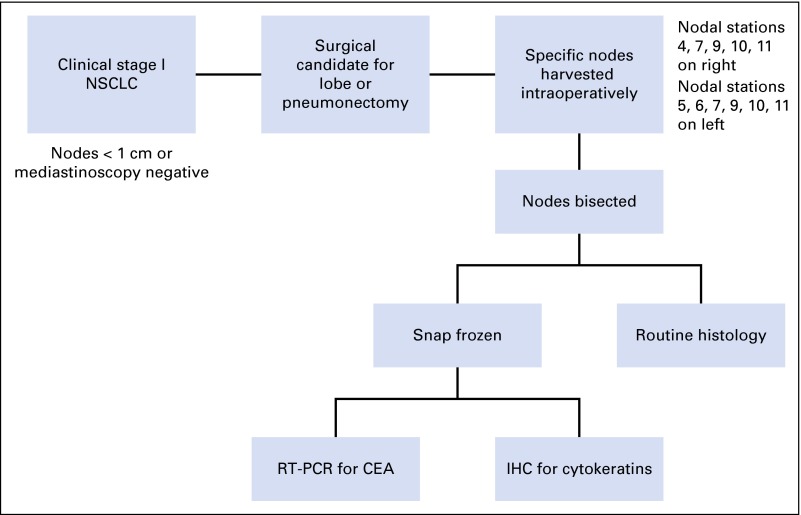
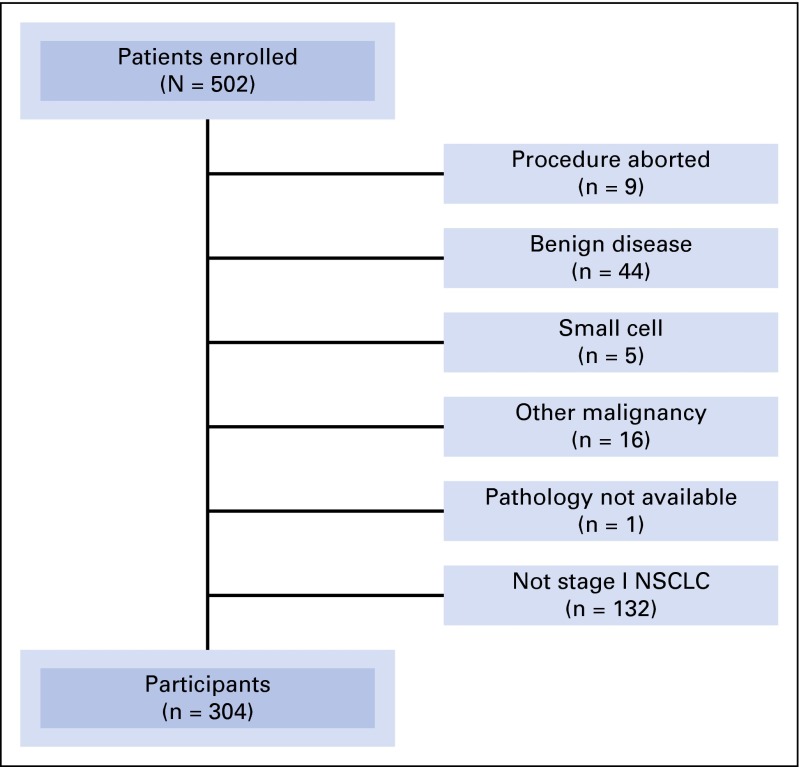
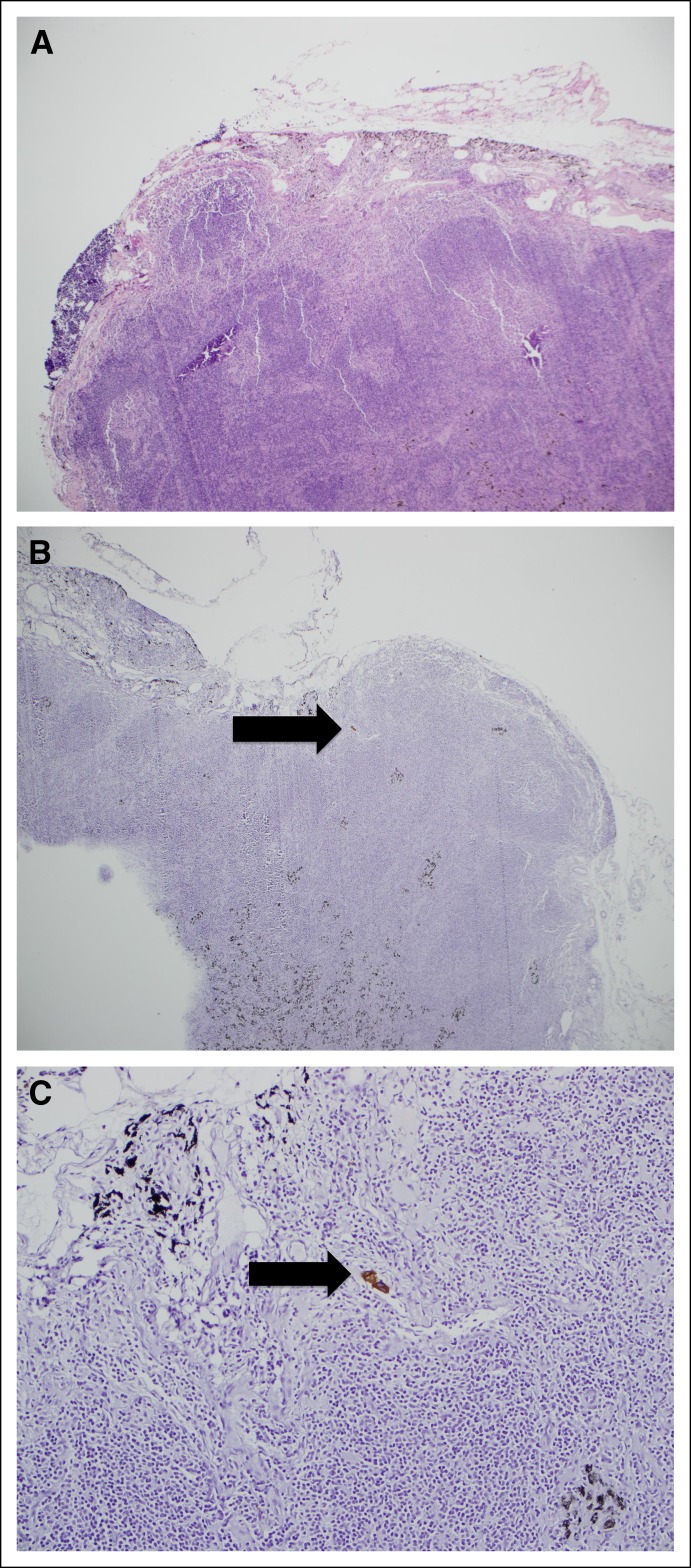
Materials and methods: Between 1997 and 2002, 502 patients with suspected clinical stage I (T1-2N0M0) NSCLC were prospectively enrolled at 11 institutions. Primary tumor and lymph nodes (LNs) were collected and sent to a central site for molecular analysis. Both were assayed for OM using immunohistochemistry (IHC) for cytokeratin (AE1/AE3) and real-time reverse transcriptase polymerase chain reaction (RT-PCR) for carcinoembryonic antigen.
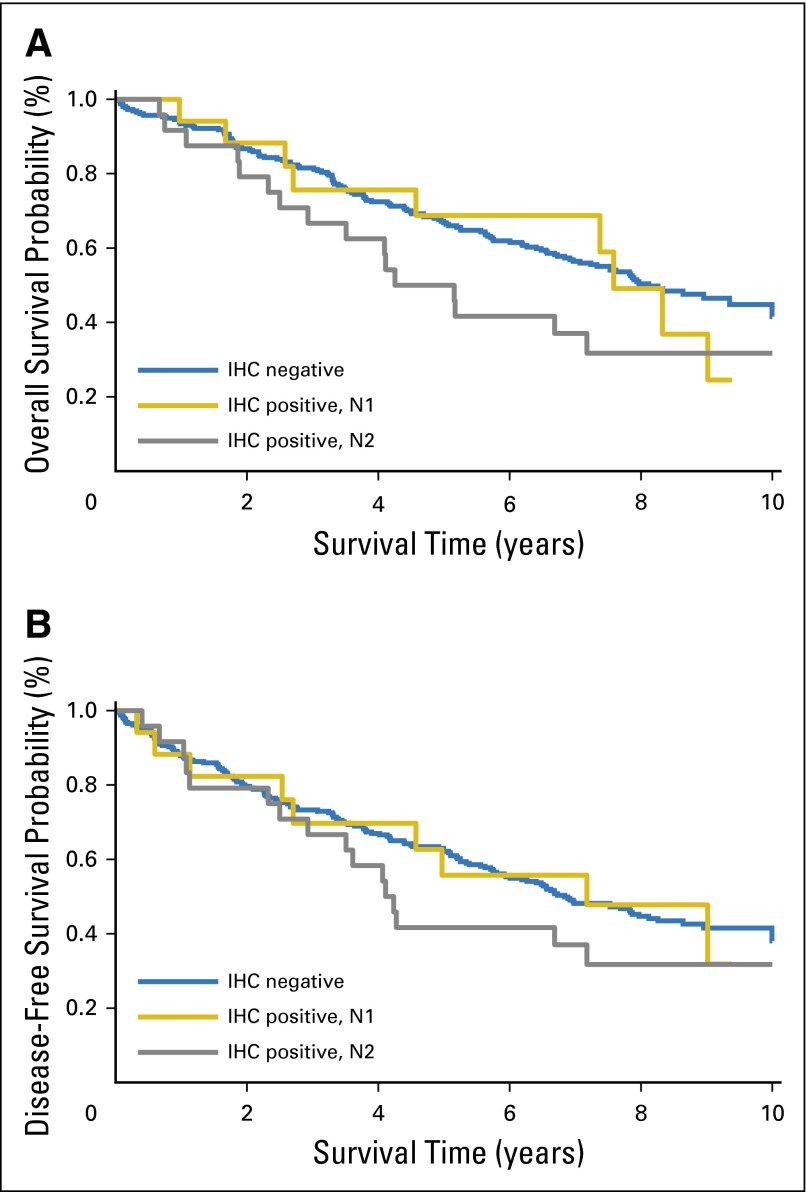
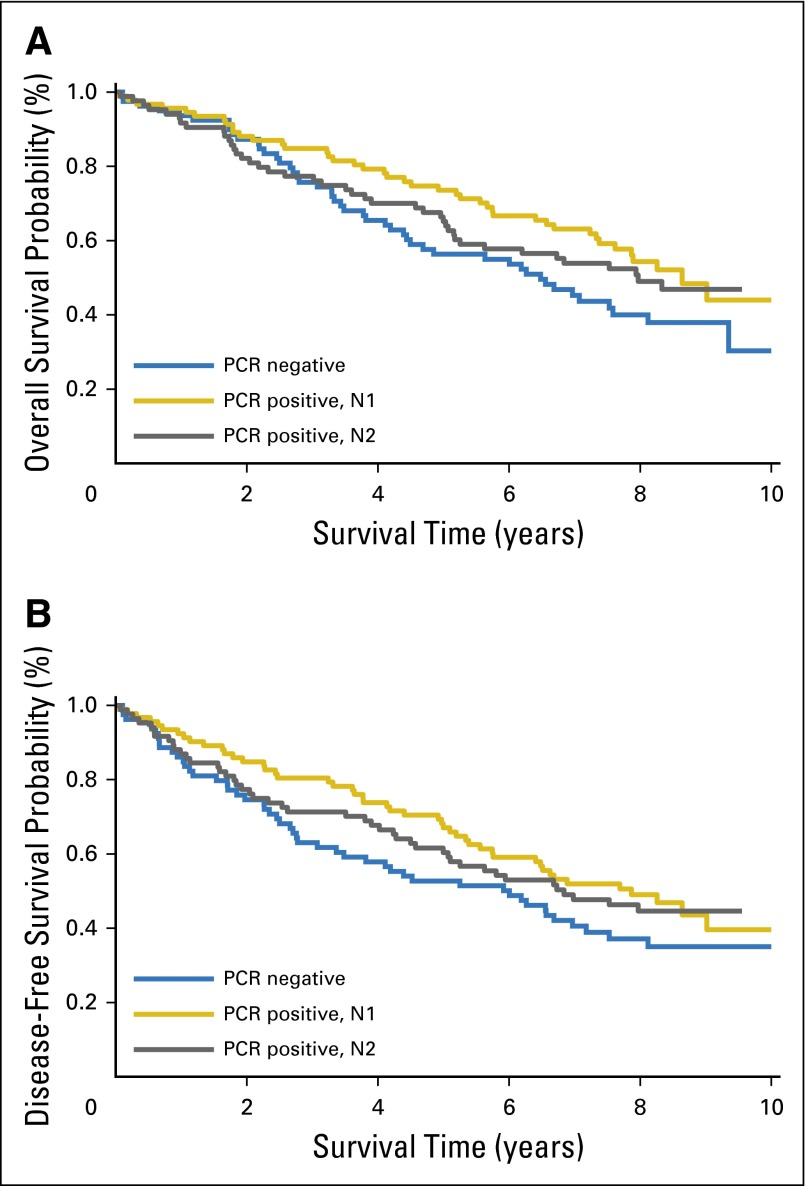
Results: Four hundred eighty-nine of the 502 enrolled patients underwent complete surgical staging. Three hundred four patients (61%) had pathologic stage I NSCLC (T1, 58%; T2, 42%) and were included in the final analysis. Fifty-six percent had adenocarcinomas, 34% had squamous cell carcinomas, and 10% had another histology. LNs from 298 patients were analyzed by IHC; 41 (14%) were IHC-positive (42% in N1 position, 58% in N2 position). Neither overall survival (OS) nor disease-free survival was associated with IHC positivity; however, patients who had IHC-positive N2 LNs had statistically significantly worse survival rates (hazard ratio, 2.04, P = .017). LNs from 256 patients were analyzed by RT-PCR; 176 (69%) were PCR-positive (52% in N1 position, 48% in N2 position). Neither OS nor disease-free survival was associated with PCR positivity.
Conclusion: NSCLC tumor markers can be detected in histologically negative LNs by AE1/AE3 IHC and carcinoembryonic antigen RT-PCR. In this prospective, multi-institutional trial, the presence of OM by IHC staining in N2 LNs of patients with NSCLC correlated with decreased OS. The clinical significance of this warrants further investigation.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
Comment in
-
Impact of lymph node occult metastases in stage I non-small cell lung cancer (NSCLC): what is the evidence?J Thorac Dis. 2016 Aug;8(8):E809-12. doi: 10.21037/jtd.2016.07.59. J Thorac Dis. 2016. PMID: 27618780 Free PMC article. No abstract available.
-
Improving post-resection risk stratification in non-small cell lung cancer: 'wit, whither wander you?'.J Thorac Dis. 2016 Sep;8(9):2315-2318. doi: 10.21037/jtd.2016.08.54. J Thorac Dis. 2016. PMID: 27746964 Free PMC article. No abstract available.
References
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2:706–714. - PubMed
-
- Koike T, Yamato Y, Yoshiya K, et al. Intentional limited pulmonary resection for peripheral T1 N0 M0 small-sized lung cancer. J Thorac Cardiovasc Surg. 2003;125:924–928. - PubMed
-
- Okada M, Koike T, Higashiyama M, et al. Radical sublobar resection for small-sized non-small cell lung cancer: A multicenter study. J Thorac Cardiovasc Surg. 2006;132:769–775. - PubMed
-
- Lou F, Huang J, Sima CS, et al. Patterns of recurrence and second primary lung cancer in early-stage lung cancer survivors followed with routine computed tomography surveillance. J Thorac Cardiovasc Surg. 2013;145:75–81, discussion 81-2. - PubMed
-
- Maeda R, Yoshida J, Ishii G, et al. Risk factors for tumor recurrence in patients with early-stage (stage I and II) non-small cell lung cancer: Patient selection criteria for adjuvant chemotherapy according to the seventh edition TNM classification. Chest. 2011;140:1494–502. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
