

Validation of the HOOS, JR: A Short-form Hip Replacement Survey
- PMID: 26926772
- PMCID: PMC4868170
- DOI: 10.1007/s11999-016-4718-2
Validation of the HOOS, JR: A Short-form Hip Replacement Survey
Abstract
Background: Patient-reported outcome measures (PROMs) are increasingly in demand for outcomes evaluation by hospitals, administrators, and policymakers. However, assessing total hip arthroplasty (THA) through such instruments is challenging because most existing measures of hip health are lengthy and/or proprietary.
Questions/purposes: The objective of this study was to derive a patient-relevant short-form survey based on the Hip disability and Osteoarthritis Outcome Score (HOOS), focusing specifically on outcomes after THA.
Methods: We retrospectively evaluated patients with hip osteoarthritis who underwent primary unilateral THA and who had completed preoperative and 2-year postoperative PROMs using our hospital's hip replacement registry. The 2-year followup in this population was 81% (4308 of 5351 patients). Of these, 2371 completed every item on the HOOS before surgery and at 2 years, making them eligible for the formal item reduction analysis. Through semistructured interviews with 30 patients, we identified items in the HOOS deemed qualitatively most important to patients with hip osteoarthritis. The original HOOS has 40 items, the four quality-of-life items were excluded a priori, five were excluded for being redundant, and one was excluded based on patient-relevance surveys. The remaining 30 items were evaluated using Rasch modeling to yield a final six-item HOOS, Joint Replacement (HOOS, JR), representing a single construct of "hip health." We calculated HOOS, JR scores for the Hospital for Special Surgery (HSS) cohort and validated this new score for internal consistency, external validity (versus HOOS and WOMAC domains), responsiveness to THA, and floor and ceiling effects. Additional external validation was performed using calculated HOOS, JR scores in collaboration with the Function and Outcomes Research for Comparative Effectiveness in Total Joint Replacement (FORCE-TJR) nationally representative joint replacement registry (n = 910).
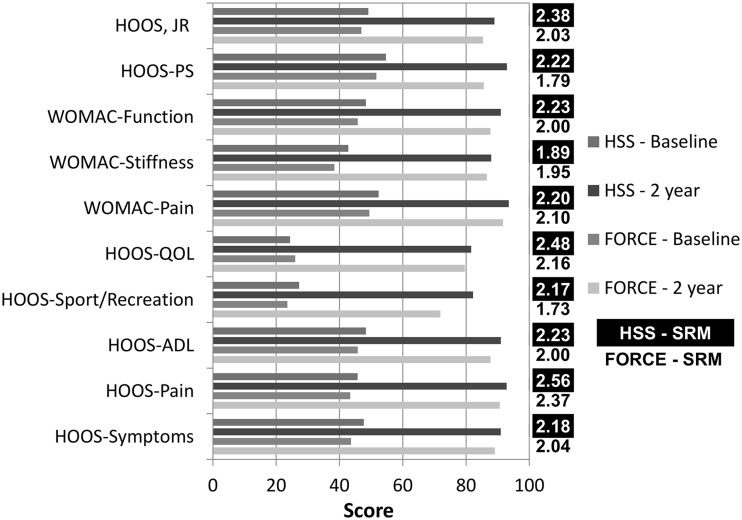
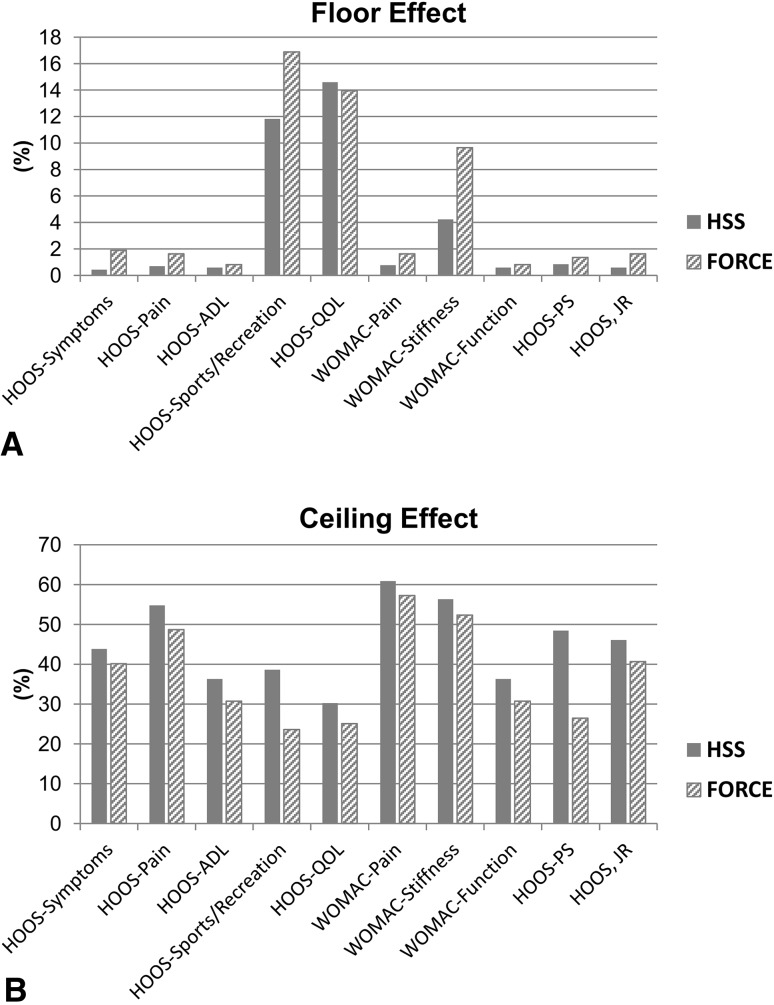
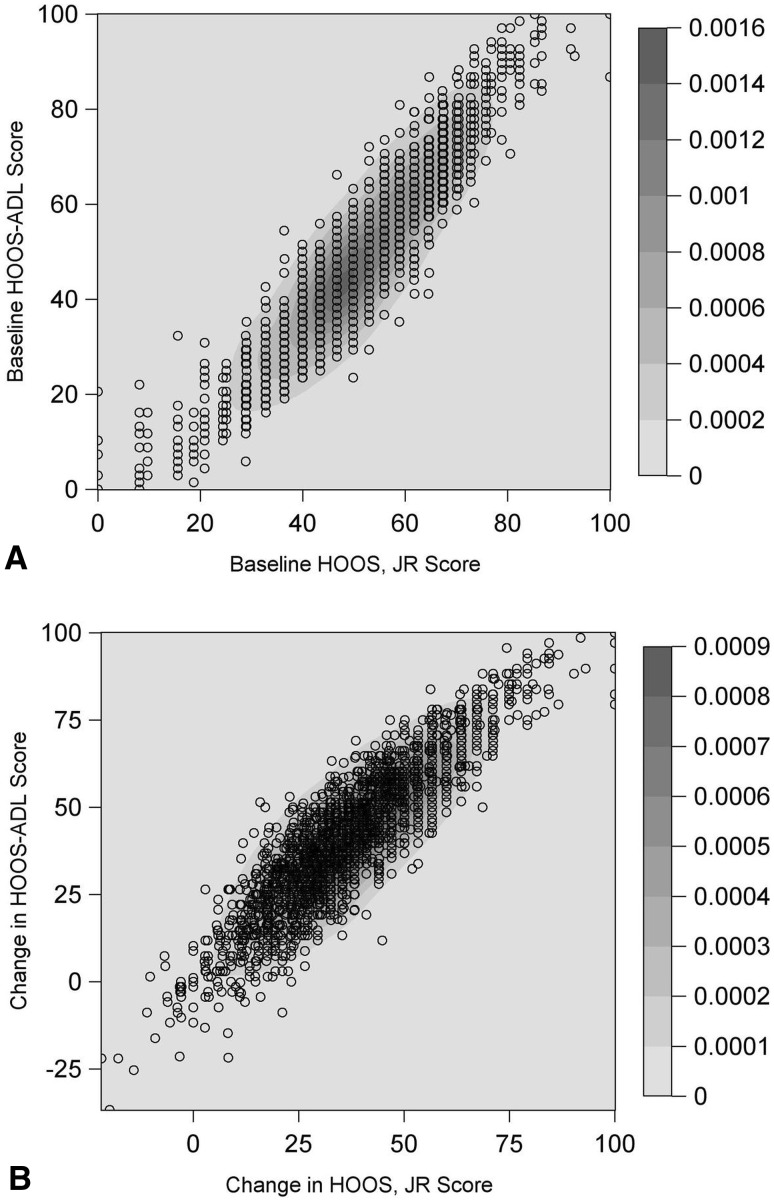
Results: The resulting six-item PROM (HOOS, JR) retained items only from the pain and activities of daily living domains. It showed high internal consistency (Person Separation Index, 0.86 [HSS]; 0.87 [FORCE]), moderate to excellent external validity against other hip surveys (Spearman's correlation coefficient, 0.60-0.94), very high responsiveness (standardized response means, 2.03 [95% CI, 1.84-2.22] [FORCE]; and 2.38 [95% CI, 2.27-2.49] [HSS]), and favorable floor (0.6%-1.9%) and ceiling (37%-46%) effects. External validity was highest for the HOOS pain (Spearman's correlation coefficient, 0.87 [95% CI, 0.86-0.89] [HSS]; and 0.87 [95% CI, 0.84-0.90] [FORCE]) and HOOS activities of daily living (Spearman's correlation coefficient, 0.94 [95% CI, 0.93-0.95] [HSS]; and 0.94 [95% CI, 0.93-0.96] [FORCE]) domains in the HSS validation cohort and the FORCE-TJR cohort.
Conclusions: The HOOS, JR provides a valid, reliable, and responsive measure of hip health for patients undergoing THA. This short-form PROM is patient relevant and efficient.
Level of evidence: Level III, diagnostic study.
Figures



References
-
- Bellamy N. WOMAC: a 20-year experiential review of a patient-centered self-reported health status questionnaire. J. Rheumatol. 2002;29:2473–2476. - PubMed
-
- Bureau of Labor Statistics. American Time Survey. Available at: http://www.bls.gov/tus/. Accessed January 12, 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
