

The Role of Aldosterone in Obesity-Related Hypertension
- PMID: 26927805
- PMCID: PMC4886496
- DOI: 10.1093/ajh/hpw003
The Role of Aldosterone in Obesity-Related Hypertension
Abstract
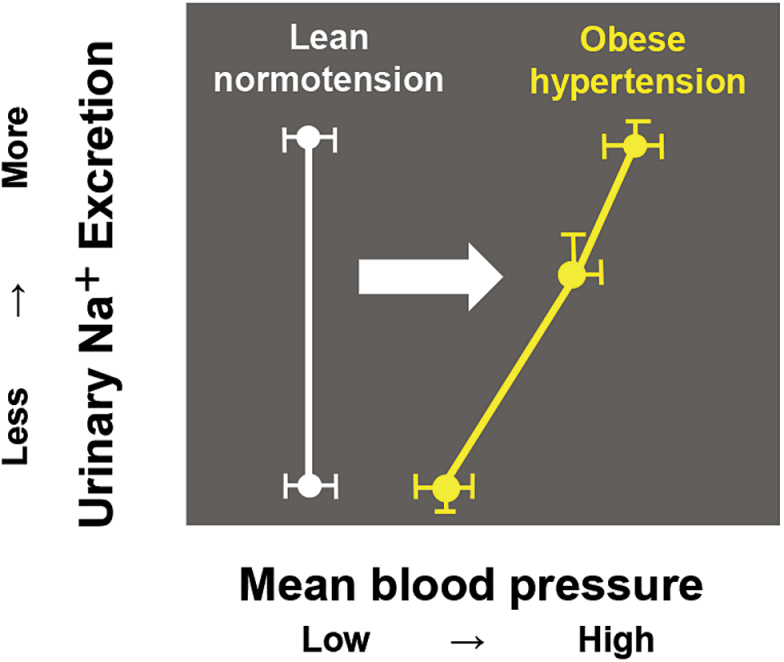
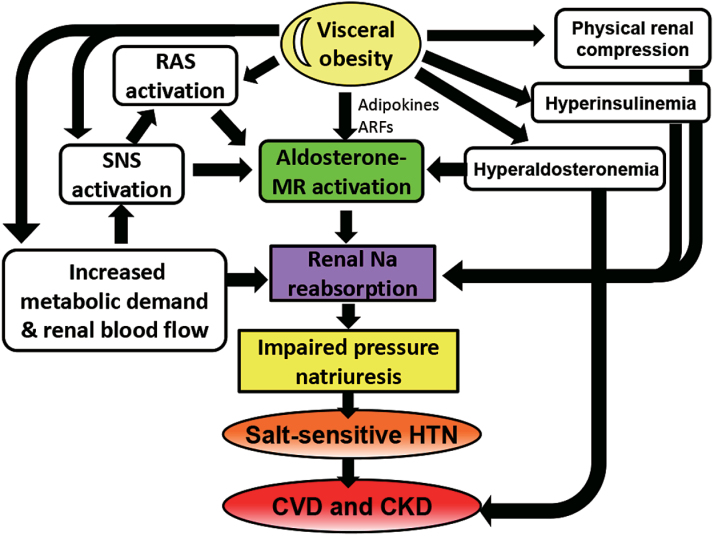
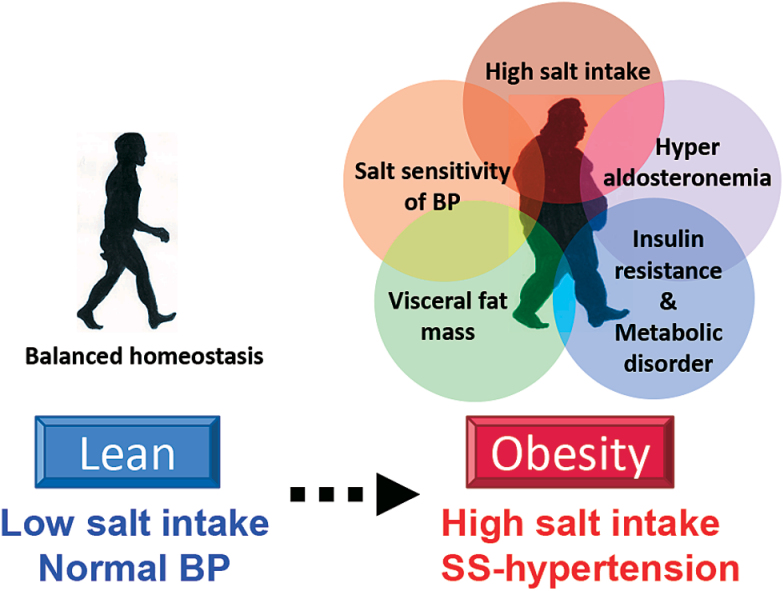
Obese subjects often have hypertension and related cardiovascular and renal diseases, and this has become a serious worldwide health problem. In obese subjects, impaired renal-pressure natriuresis causes sodium retention, leading to the development of salt-sensitive hypertension. Physical compression of the kidneys by visceral fat and activation of the sympathetic nervous system, renin-angiotensin systems (RAS), and aldosterone/mineralocorticoid receptor (MR) system are involved in this mechanism. Obese subjects often exhibit hyperaldosteronism, with increased salt sensitivity of blood pressure (BP). Adipose tissue excretes aldosterone-releasing factors, thereby stimulating aldosterone secretion independently of the systemic RAS, and aldosterone/MR activation plays a key role in the development of hypertension and organ damage in obesity. In obese subjects, both salt sensitivity of BP, enhanced by obesity-related metabolic disorders including aldosterone excess, and increased dietary sodium intake are closely related to the incidence of hypertension. Some salt sensitivity-related gene variants affect the risk of obesity, and together with salt intake, its combination is possibly associated with the development of hypertension in obese subjects. With high salt levels common in modern diets, salt restriction and weight control are undoubtedly important. However, not only MR blockade but also new diagnostic modalities and therapies targeting and modifying genes that are related to salt sensitivity, obesity, or RAS regulation are expected to prevent obesity and obesity-related hypertension.
Keywords: aldosterone; blood pressure; hypertension; obesity; salt; salt sensitivity of blood pressure..
© American Journal of Hypertension, Ltd 2016. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Withrow D, Alter DA. The economic burden of obesity worldwide: a systematic review of the direct costs of obesity. Obes Rev 2011; 12:131–141. - PubMed
-
- Müller-Riemenschneider F, Reinhold T, Berghöfer A, Willich SN. Health-economic burden of obesity in Europe. Eur J Epidemiol 2008; 23:499–509. - PubMed
-
- Must A, Spadano J, Coakley EH, Field AE, Colditz G, Dietz WH. The disease burden associated with overweight and obesity. JAMA 1999; 282:1523–1529. - PubMed
-
- Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation 1983; 67:968–977. - PubMed
-
- Burton BT, Foster WR, Hirsch J, Van Itallie TB. Health implications of obesity: an NIH Consensus Development Conference. Int J Obes 1985; 9:155–170. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
