

Characterizing a psychiatric symptom dimension related to deficits in goal-directed control
- PMID: 26928075
- PMCID: PMC4786435
- DOI: 10.7554/eLife.11305
Characterizing a psychiatric symptom dimension related to deficits in goal-directed control
Abstract
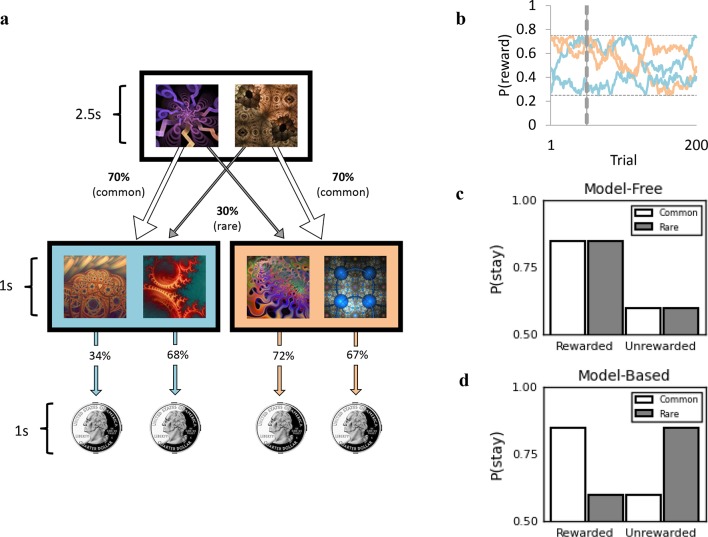
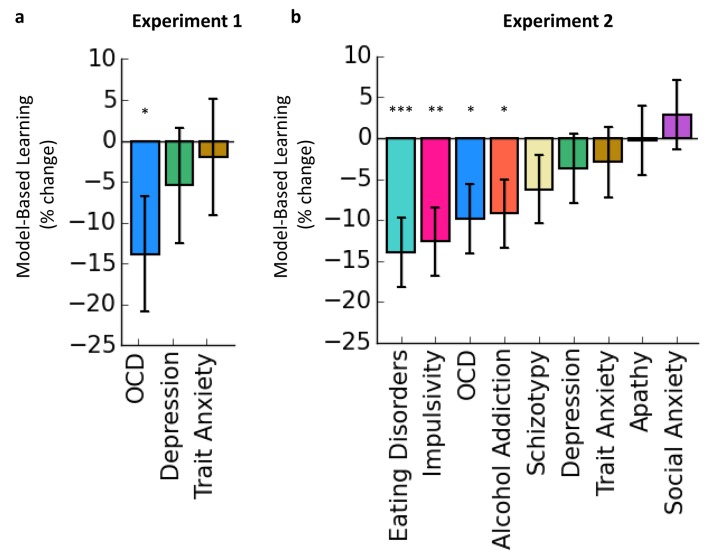
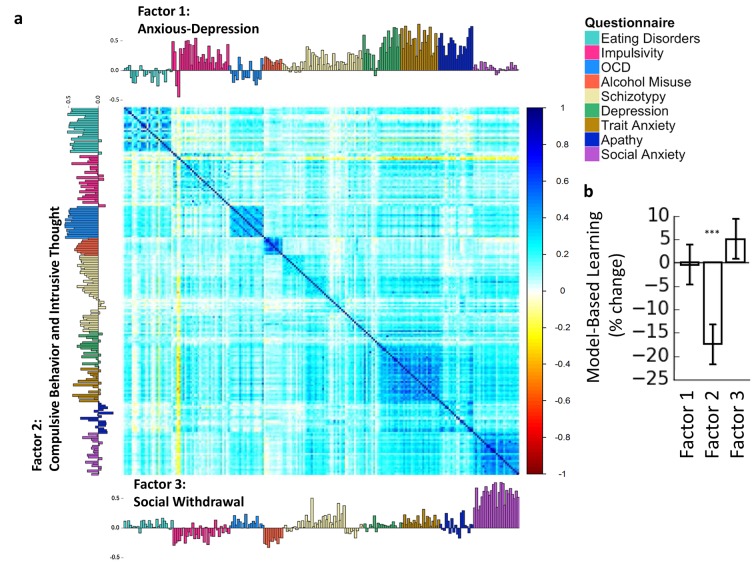
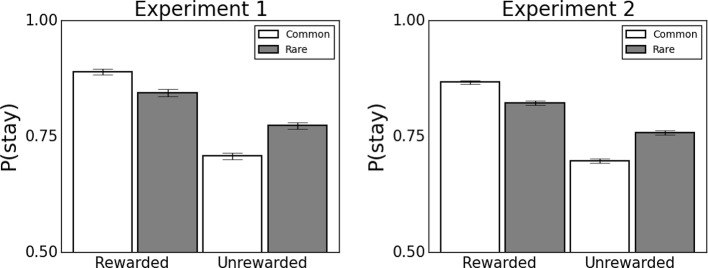
Prominent theories suggest that compulsive behaviors, characteristic of obsessive-compulsive disorder and addiction, are driven by shared deficits in goal-directed control, which confers vulnerability for developing rigid habits. However, recent studies have shown that deficient goal-directed control accompanies several disorders, including those without an obvious compulsive element. Reasoning that this lack of clinical specificity might reflect broader issues with psychiatric diagnostic categories, we investigated whether a dimensional approach would better delineate the clinical manifestations of goal-directed deficits. Using large-scale online assessment of psychiatric symptoms and neurocognitive performance in two independent general-population samples, we found that deficits in goal-directed control were most strongly associated with a symptom dimension comprising compulsive behavior and intrusive thought. This association was highly specific when compared to other non-compulsive aspects of psychopathology. These data showcase a powerful new methodology and highlight the potential of a dimensional, biologically-grounded approach to psychiatry research.
Keywords: compulsive; computational; dimensional; goal-directed; habit; human; human biology; medicine; neuroscience; psychiatry.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures
References
-
- American Psychiatric Association . (5 edn) American Psychiatric Publishing; 2013. Diagnostic and Statistical Manual of Mental Disorders.
-
- Baker F. Marcel Dekker; 1992. Item Response Theory: Parameter Estimation Techniques.
-
- Bezanson J, Karpinski S, Shah VB, Edelman A. Julia: a fast dynamic language for technical computing. MIT 2012
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
