

Synergistic association of combined glycemic and blood pressure level with risk of complications in US veterans with diabetes
- PMID: 26928222
- PMCID: PMC5705006
- DOI: 10.1097/HJH.0000000000000864
Synergistic association of combined glycemic and blood pressure level with risk of complications in US veterans with diabetes
Abstract
Objectives: Hemoglobin A1c levels less than 7.0% and systolic blood pressure (SBP) less than 140 mmHg are each associated with lower risk of vascular complications in patients with diabetes mellitus. Associations between combined A1c level and SBP categories and risk of mortality and morbidity in diabetic patients are not well characterized.
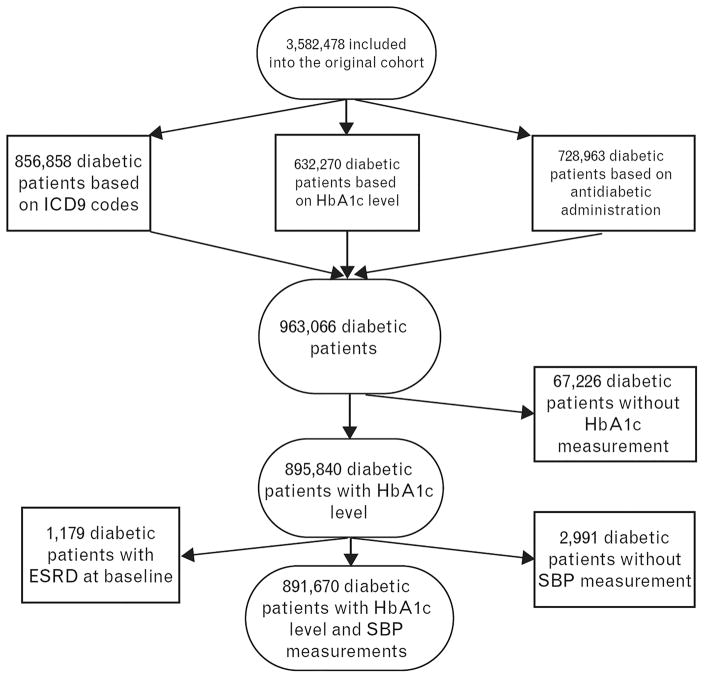
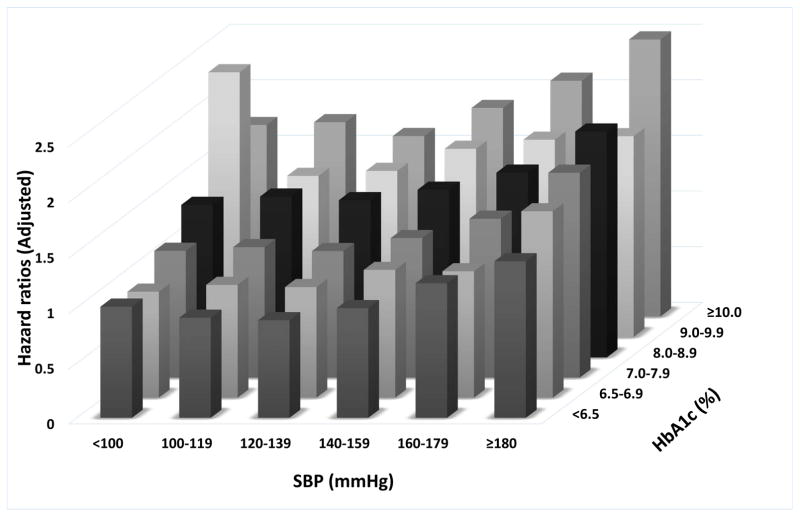
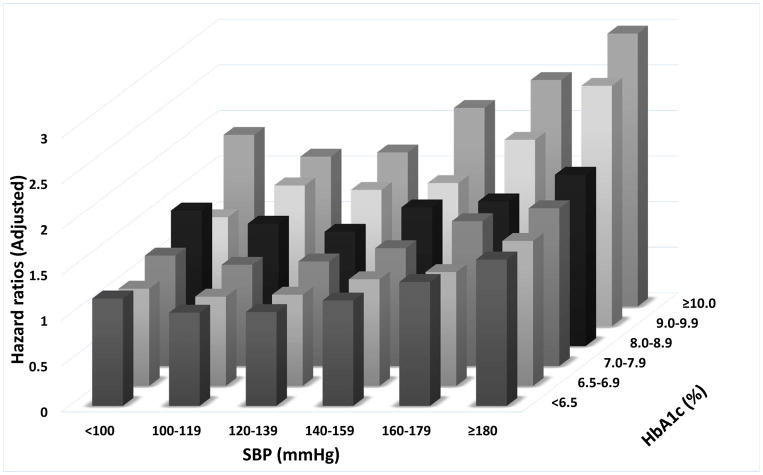
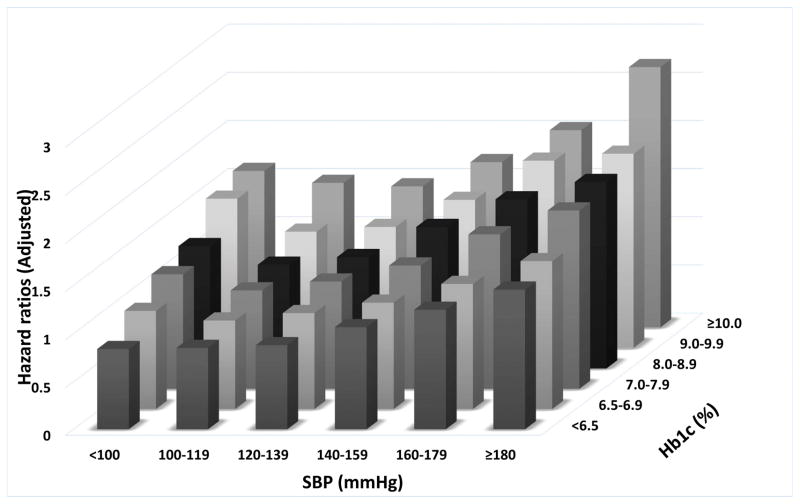
Methods: We examined 891 670 US diabetic veterans with baseline estimated glomerular filtration rates more than 60 ml/min per 1.73 m (mean age 67 ± 11 years, 97% men, 17% African-Americans). The associations of mutually exclusive combined categories of A1c (<6.5, 6.5-6.9, 7.0-7.9, 8.0-8.9, 9.0-9.9, and ≥10%) and SBP (<100, 100-119, 120-139, 140-159, 160-179, and ≥180 mmHg) with the risk of all-cause mortality and incident chronic kidney disease (CKD), coronary heart disease, and stroke were examined in Cox models adjusted for baseline characteristics using patients with concomitant A1c 6.5-6.9% and SBP of 120-139 mmHg as the referent group.
Results: A total of 221 529 (25%) patients died, and 178 588 (20%), 43 373 (5%) and 36 935 (4%) developed CKD, coronary heart disease and stroke, respectively, during a median follow-up of 7.4 years. SBP displayed a J-shaped association with each outcome except CKD risk that was linearly associated with SBP across all A1c categories. A1c above 7.0% was associated with monotonically worse outcomes for all end points in all SBP categories. Patients with the combined highest A1c and SBP levels experienced the worst outcomes.
Conclusion: SBP greater than 120-139 mmHg and A1c greater than 7.0% are associated with higher mortality and vascular complications in diabetic patients, independent of each other. Combined efforts to improve both glycemic and blood pressure control may synergistically improve outcomes in patients with normal kidney function.
Conflict of interest statement
ARG reports personal fees from AstraZeneca and Janssen Pharmaceutical and grant support from Sanofi and Novo Nordisk paid to the UTHSC, Memphis. MZM reports support from Czech Health Research Council, outside the submitted work. KK-Z reports personal fees from Abbott, AbbVie, Amgen, Fresenius, Genentech, Genzyme–Sanofi, Hospira, Keryx, Shire, and Vifor, non-financial support from DaVita, and grants from the US National Institutes of Health (NIH), outside the submitted work. CPK reports personal fees from Amgen, NPS, Relypsa, ZS Pharma, and Sanofi-Aventis, royalties from UpToDate for a review article about metabolic acidosis, and grants from the NIH, AbbVie, Amgen, OPKO, and Shire, outside the submitted work. CPK and KK-Z are employees of the US Department of Veterans Affairs and their opinions expressed in this paper are those of the authors’ and do not necessarily represent the opinion of the Department of Veterans Affairs. The other authors declare no competing interests.
Figures

Comment in
-
High blood pressure in US diabetic veterans with normal renal function: a plea for the design of a more powerful and conclusive outcome trial.J Hypertens. 2016 May;34(5):836-7. doi: 10.1097/HJH.0000000000000896. J Hypertens. 2016. PMID: 27027378 No abstract available.
References
-
- American Diabetes A. Standards of medical care in diabetes--2014. Diabetes care. 2014;37(Suppl 1):S14–80. - PubMed
-
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837–53. - PubMed
-
- Reichard P, Nilsson BY, Rosenqvist U. The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus. The New England journal of medicine. 1993;329(5):304–9. - PubMed
-
- The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. The New England journal of medicine. 1993;329(14):977–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
