

Autoimmune Bullous Skin Disorders with Immune Checkpoint Inhibitors Targeting PD-1 and PD-L1
- PMID: 26928461
- PMCID: PMC5241697
- DOI: 10.1158/2326-6066.CIR-15-0123
Autoimmune Bullous Skin Disorders with Immune Checkpoint Inhibitors Targeting PD-1 and PD-L1
Abstract
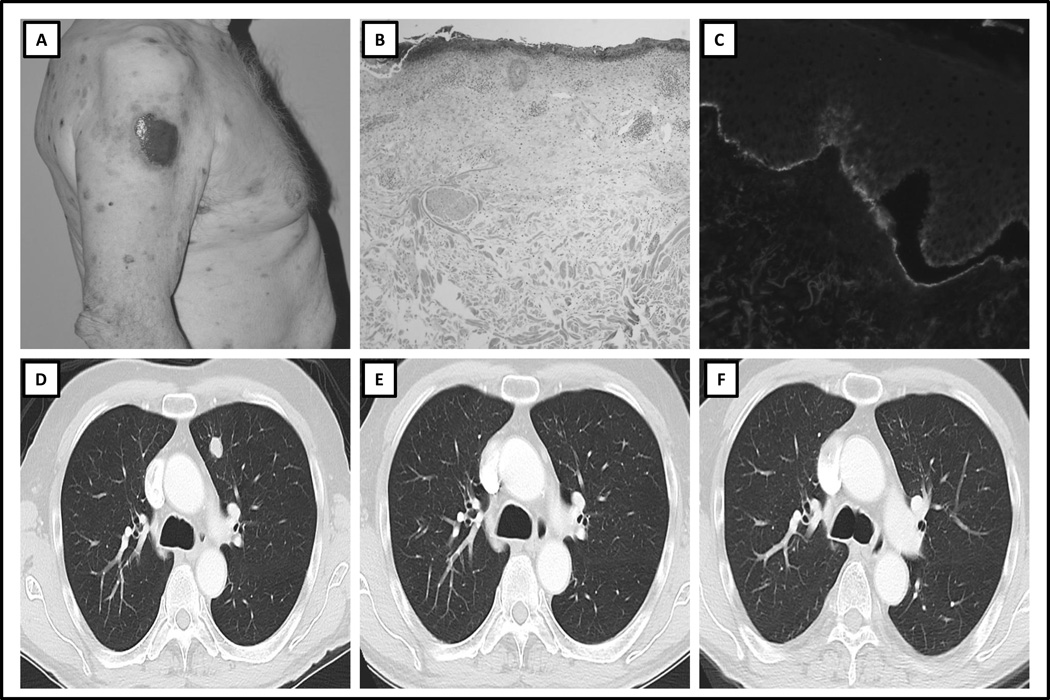
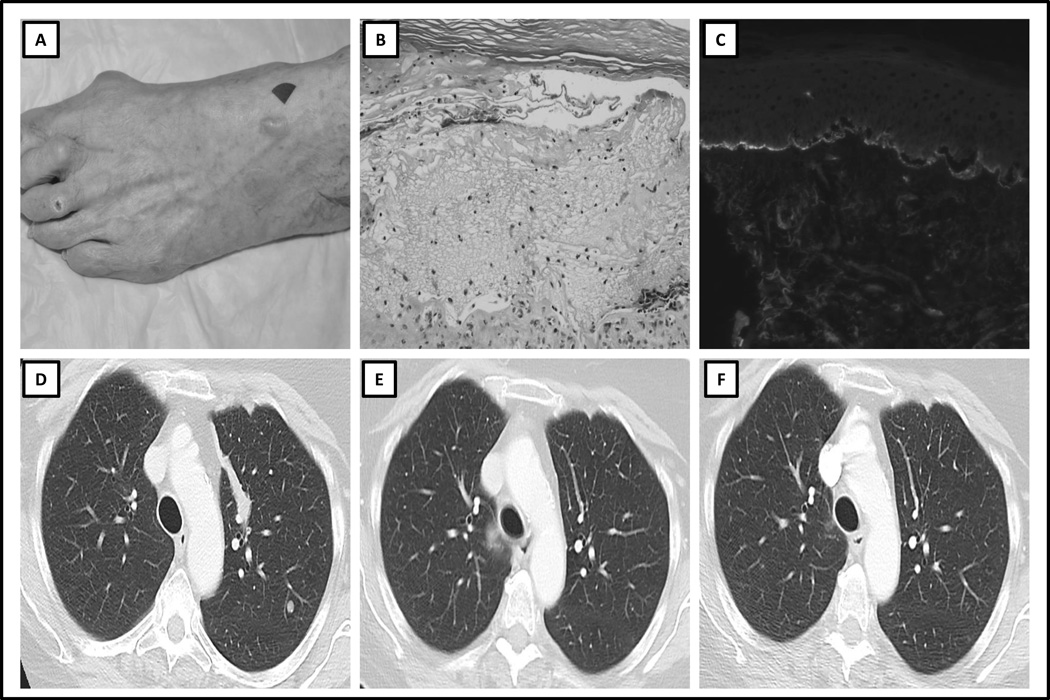
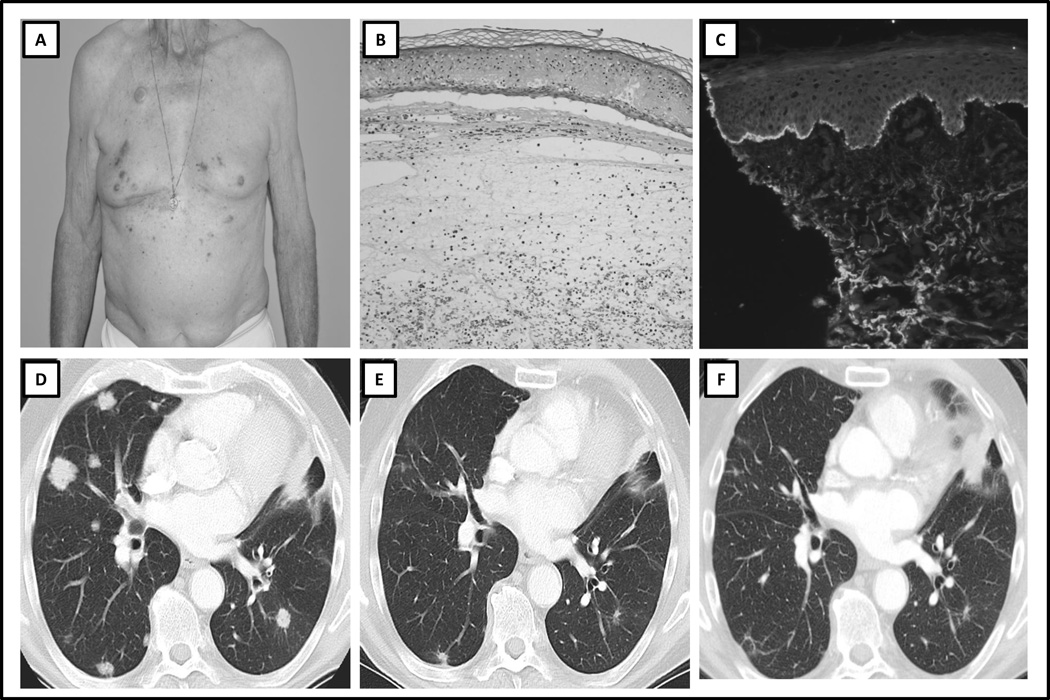
Monoclonal antibodies (mAb) targeting immune checkpoint pathways such as cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed death 1 (PD-1) may confer durable disease control in several malignancies. In some patients, immune checkpoint mAbs cause cutaneous immune-related adverse events. Although the most commonly reported cutaneous toxicities are mild, a subset may persist despite therapy and can lead to severe or life-threatening toxicity. Autoimmune blistering disorders are not commonly associated with immune checkpoint mAb therapy. We report a case series of patients who developed bullous pemphigoid (BP), an autoimmune process classically attributed to pathologic autoantibody formation and complement deposition. Three patients were identified. Two patients developed BP while receiving the anti-PD-1 mAb nivolumab, and one while receiving the anti-PD-L1 mAb durvalumab. The clinicopathologic features of each patient and rash, and corresponding radiologic findings at the development of the rash and after its treatment, are described. Patients receiving an anti-PD-1/PD-L1 mAb may develop immune-related BP. This may be related to both T-cell- and B-cell-mediated responses. Referral to a dermatologist for accurate diagnosis and management is recommended. Cancer Immunol Res; 4(5); 383-9. ©2016 AACR.
©2016 American Association for Cancer Research.
Conflict of interest statement
JN, KS, CAQ, KB, JC, DBP, AW, ASL, EAQ, PKP, MD, SPA : No relevant disclosures
Figures
References
-
- Robert C, Thomas L, Bondarenko I, O'Day S, M DJ, Garbe C, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. The New England journal of medicine. 2011 Jun 30;364(26):2517–2526. PubMed PMID: 21639810. Epub 2011/06/07. eng. - PubMed
-
- Minkis K, Garden BC, Wu S, Pulitzer MP, Lacouture ME. The risk of rash associated with ipilimumab in patients with cancer: a systematic review of the literature and meta-analysis. Journal of the American Academy of Dermatology. 2013 Sep;69(3):e121–e128. PubMed PMID: 23357570. Epub 2013/01/30. eng. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
