

Adult height, nutrition, and population health
- PMID: 26928678
- PMCID: PMC4892290
- DOI: 10.1093/nutrit/nuv105
Adult height, nutrition, and population health
Abstract
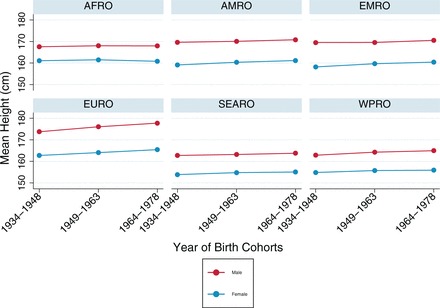
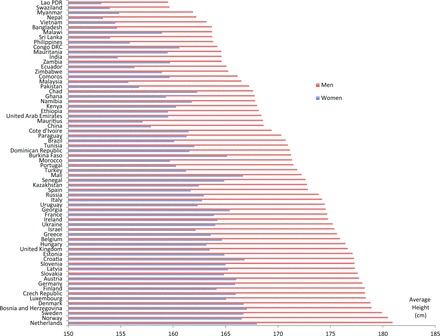
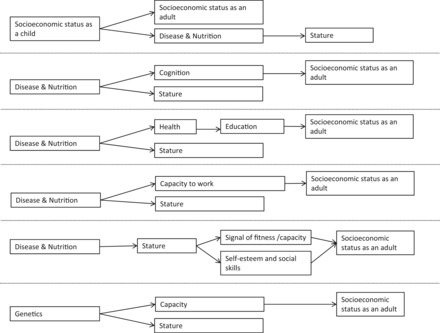
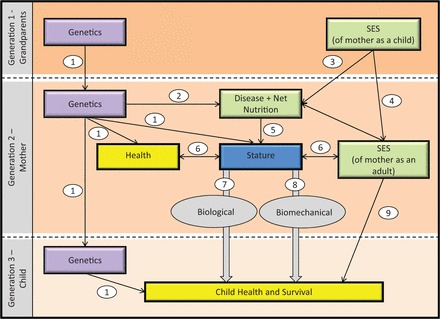
In this review, the potential causes and consequences of adult height, a measure of cumulative net nutrition, in modern populations are summarized. The mechanisms linking adult height and health are examined, with a focus on the role of potential confounders. Evidence across studies indicates that short adult height (reflecting growth retardation) in low- and middle-income countries is driven by environmental conditions, especially net nutrition during early years. Some of the associations of height with health and social outcomes potentially reflect the association between these environmental factors and such outcomes. These conditions are manifested in the substantial differences in adult height that exist between and within countries and over time. This review suggests that adult height is a useful marker of variation in cumulative net nutrition, biological deprivation, and standard of living between and within populations and should be routinely measured. Linkages between adult height and health, within and across generations, suggest that adult height may be a potential tool for monitoring health conditions and that programs focused on offspring outcomes may consider maternal height as a potentially important influence.
Keywords: genetics; height; intergenerational; life course; morbidity; mortality; nutrition; population health; socioeconomic status; stature.
© The Author(s) 2016. Published by Oxford University Press on behalf of the International Life Sciences Institute. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- Villermé LR. Mémoire sur la taille de l'homme en France. Annales d'Hygiène Publique et de Médicine Légale. 1829;1:351–396.
-
- Tanner JM. A History of the Study of Human Growth. Cambridge, UK: Cambridge University Press; 1981.
-
- Coelho PRP, McGuire RA. Diets versus diseases: the anthropometrics of slave children. J Econ Hist. 2000;60:232–246. - PubMed
-
- Steckel RH. Diets versus diseases in the anthropometrics of slave children: a reply. J Econ Hist. 2000;60:247–259. - PubMed
-
- Carson SA. Geography, insolation, and vitamin D in nineteenth century US African-American and white statures. Explor Econ Hist. 2009;46:149–159.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
