

Tofacitinib or adalimumab versus placebo: patient-reported outcomes from a phase 3 study of active rheumatoid arthritis
- PMID: 26929445
- PMCID: PMC4870388
- DOI: 10.1093/rheumatology/kev442
Tofacitinib or adalimumab versus placebo: patient-reported outcomes from a phase 3 study of active rheumatoid arthritis
Abstract
Objective: To evaluate effects of tofacitinib or adalimumab on patient-reported outcomes (PROs) in patients with moderate to severe RA and inadequate responses to MTX.
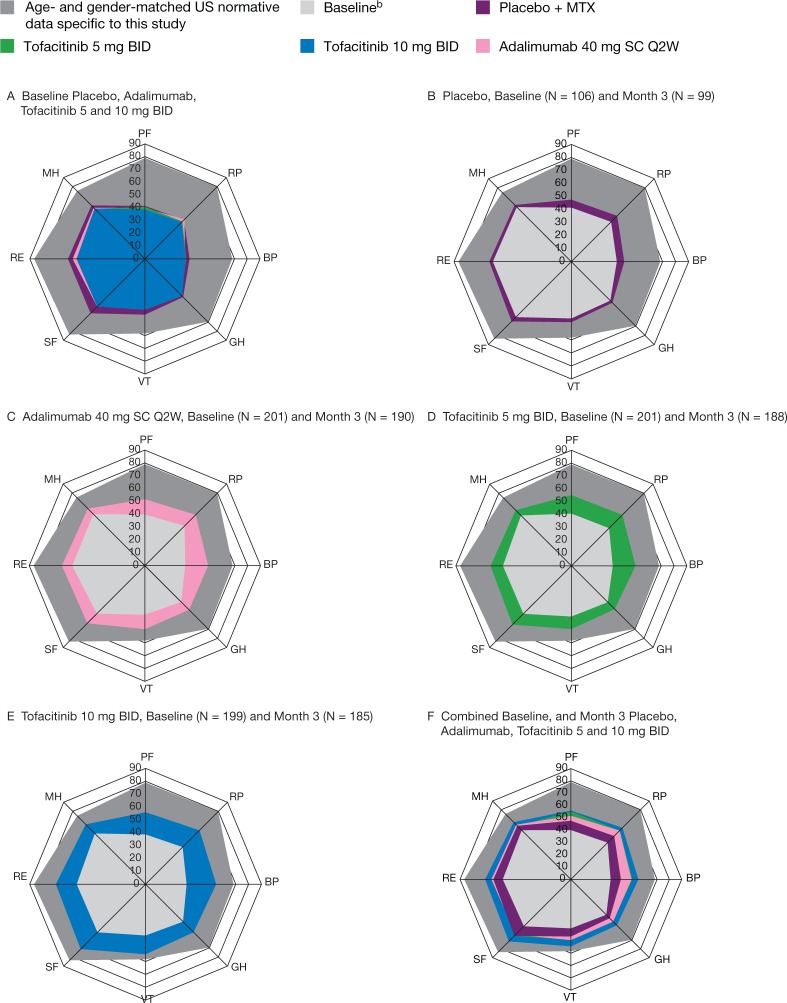
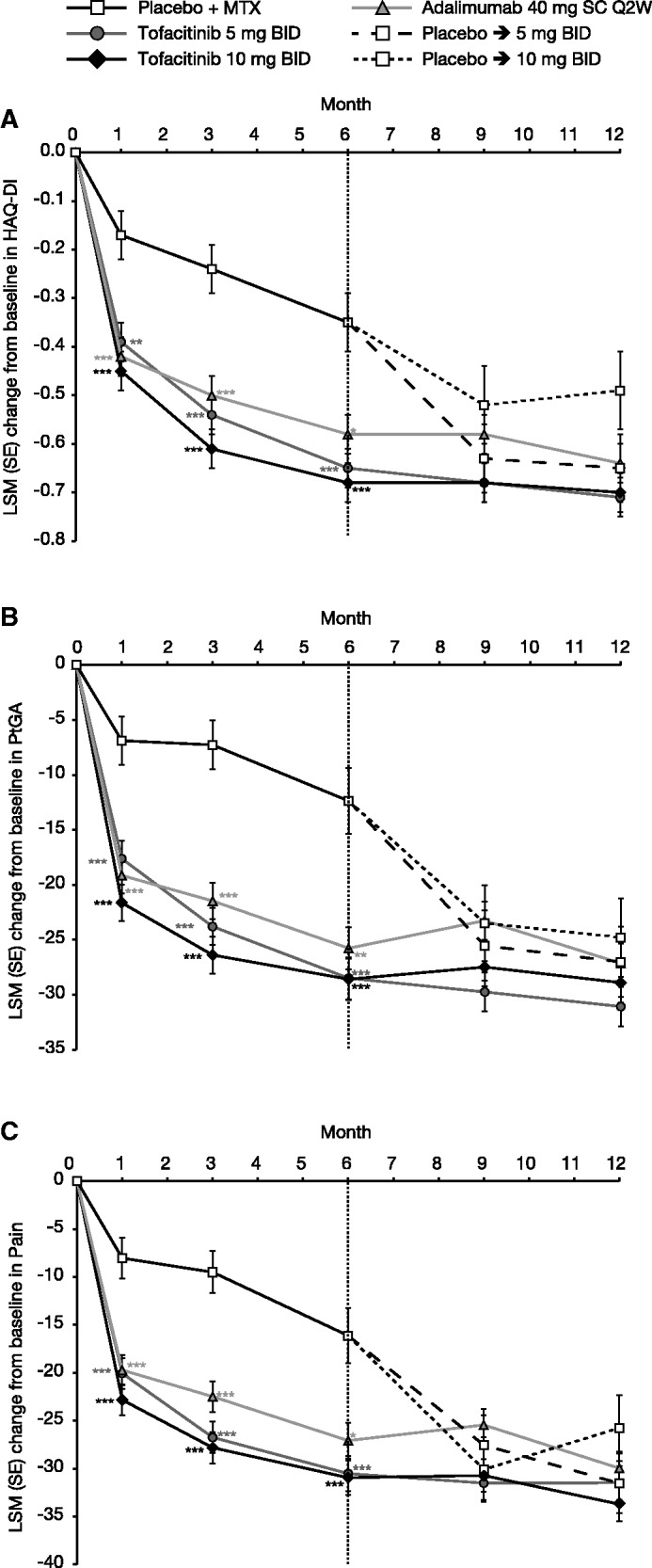
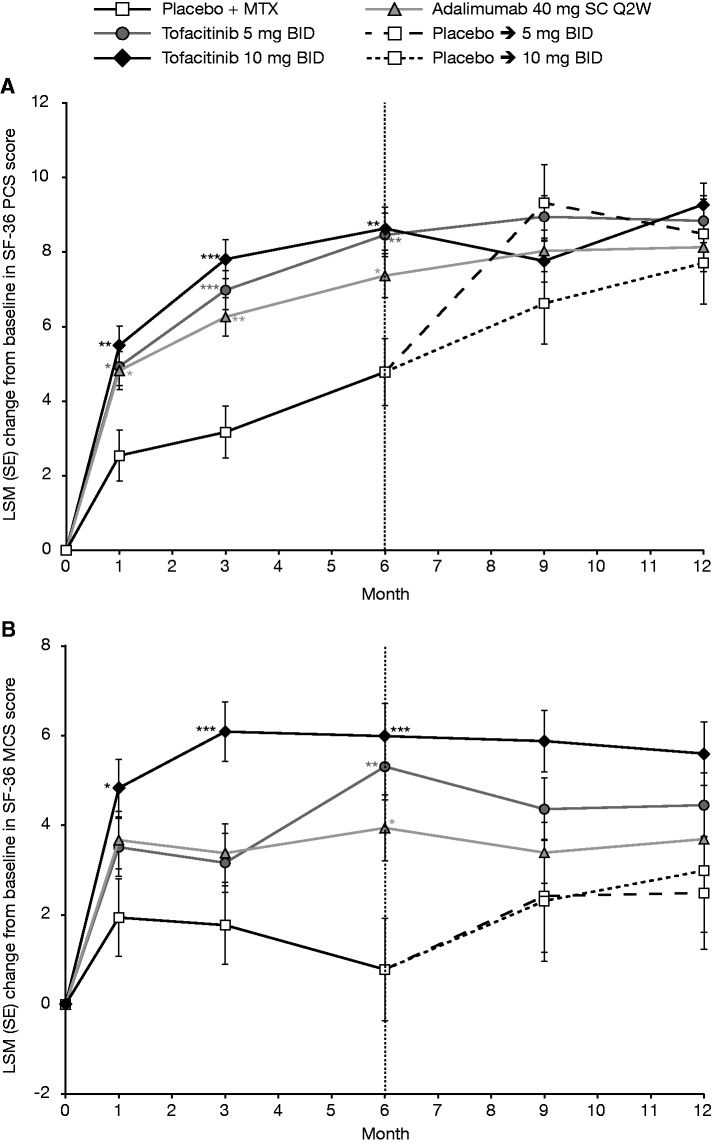
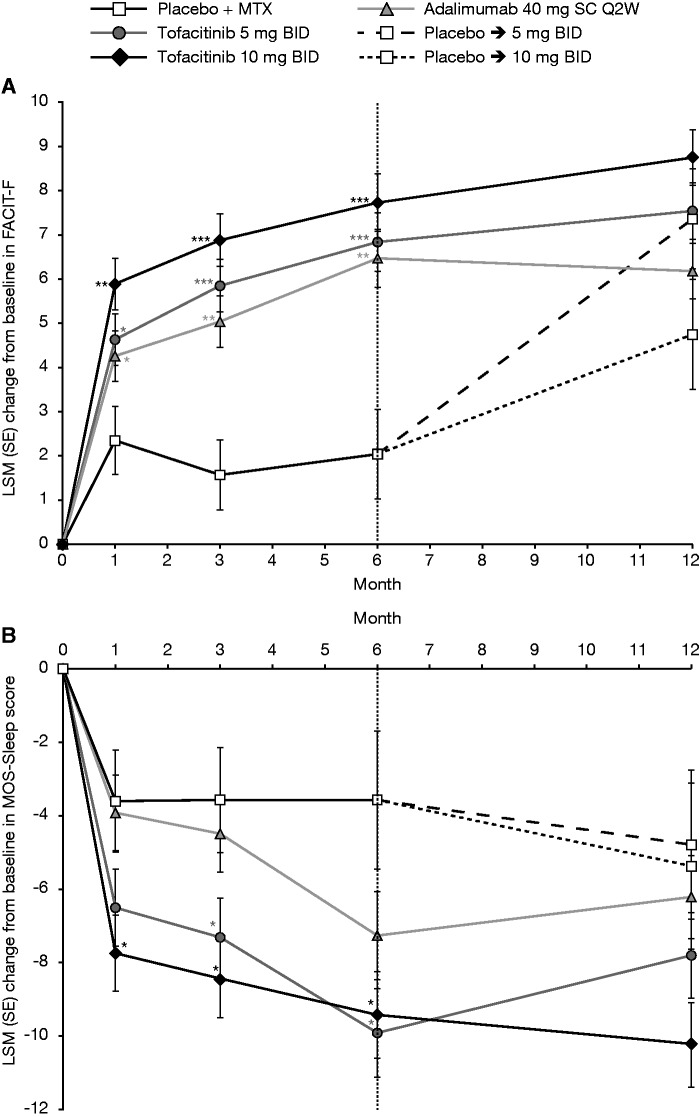
Methods: In this 12-month, phase 3, randomized controlled trial (ORAL Standard), patients (n = 717) receiving background MTX were randomized to tofacitinib 5 or 10 mg twice daily (BID), adalimumab 40 mg once every 2 weeks or placebo. PROs included HAQ-Disability Index, Patient Global Assessment of Arthritis, Patient Assessment of Arthritis Pain, health-related quality of life (Short Form-36 [SF-36]), fatigue (Functional Assessment of Chronic Illness Therapy-Fatigue) and sleep (Medical Outcomes Study-Sleep).
Results: At month 3, tofacitinib 10 mg BID treatment resulted in significant changes from baseline vs placebo across all PROs, sustained to month 12, with the highest number of patients reporting improvements ⩾minimum clinically important differences vs placebo (P < 0.05). Changes from baseline at month 3 with tofacitinib 5 mg BID and adalimumab were similar and statistically significant vs placebo across most PROs, excluding SF-36 Mental Component Score and Social Functioning, Role Emotional, and Mental Health domains, with significantly more patients reporting improvements ⩾minimum clinically important differences. Numbers Needed to Treat were lowest for tofacitinib 10 mg BID and similar between tofacitinib 5 mg BID and adalimumab.
Conclusion: Patients with moderate to severe RA and inadequate responses to MTX reported improvements across a broad range of PROs with tofacitinib 5 and 10 mg BID and adalimumab that were significantly superior to placebo.
Keywords: Janus kinase; patient-reported outcomes; phase 3; rheumatoid arthritis; tofacitinib.
© The Author 2016. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
References
-
- Kosinski M, Kujawski SC, Martin R. et al. Health-related quality of life in early rheumatoid arthritis: impact of disease and treatment response. Am J Manag Care 2002;8:231–40. - PubMed
-
- Strand V, Singh JA. Newer biological agents in rheumatoid arthritis: impact on health-related quality of life and productivity. Drugs 2010;70:121–45. - PubMed
-
- Matcham F, Scott IC, Rayner L. et al. The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: a systematic review and meta-analysis. Semin Arthritis Rheum 2014;44:123–30. - PubMed
-
- Wolfe F, Michaud K, Li T. Sleep disturbance in patients with rheumatoid arthritis: evaluation by medical outcomes study and visual analog sleep scales. J Rheumatol 2006;33:1942–51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
