

Cardiovascular risk assessment in the treatment of nonalcoholic steatohepatitis: a secondary analysis of the MOZART trial
- PMID: 26929777
- PMCID: PMC4749859
- DOI: 10.1177/1756283X15621232
Cardiovascular risk assessment in the treatment of nonalcoholic steatohepatitis: a secondary analysis of the MOZART trial
Abstract
Background: Nonalcoholic steatohepatitis (NASH) is associated with increased cardiovascular risk and mortality. No US Food and Drug Administration (FDA) approved therapies for NASH are available; clinical trials to date have not yet systematically assessed for changes in cardiovascular risk. This study examines the prospective utility of cardiovascular risk assessments, the Framingham risk score (FRS) and coronary artery calcium (CAC) score, as endpoints in a NASH randomized clinical trial, and assesses whether histologic improvements lead to lower cardiovascular risk.
Methods: Secondary analysis of a 24-week randomized, double-blind, placebo-controlled trial (MOZART) in which 50 biopsy-proven NASH patients received oral ezetimibe 10 mg daily (n = 25) versus placebo (n = 25). Biochemical profiling, FRS, CAC scores, liver biopsies were obtained at baseline and endpoint.
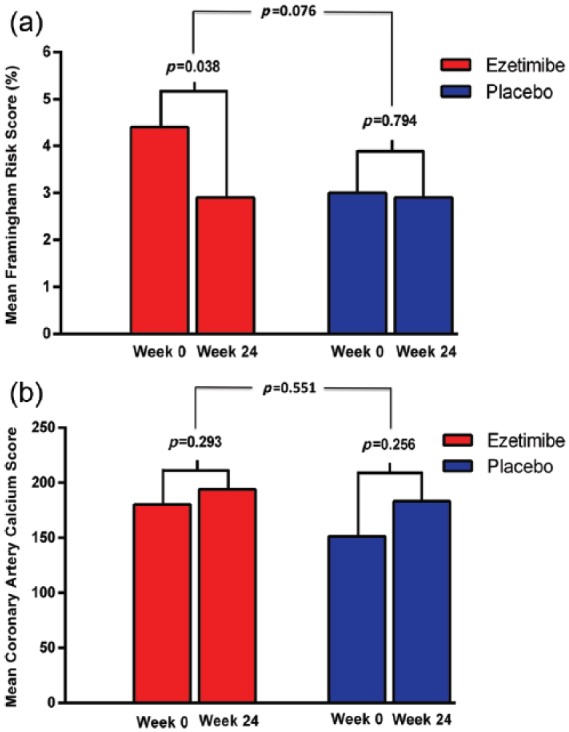
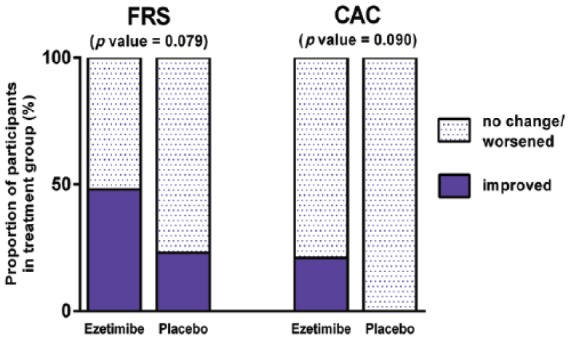
Results: Ezetimibe improved FRS whereas placebo did not (4.4 ± 6.2 to 2.9 ± 4.8, p = 0.038; 3.0 ± 4.4 to 2.9 ± 4.2, p = 0.794). CAC scores did not change with ezetimibe or placebo (180.4 ± 577.2 to 194.1 ± 623.9, p = 0.293; 151.4 ± 448.9 to 183.3 ± 555.7, p = 0.256). Ezetimibe improved FRS and CAC scores in more patients than placebo (48% versus 23%, p = 0.079, and 21% versus 0%, p = 0.090, respectively), though not significantly. No differences were noted in cardiovascular risk scores among histologic responders versus nonresponders.
Conclusions: Ezetimibe improved FRS whereas placebo did not. FRS and CAC scores improved in a greater proportion of patients with ezetimibe; this trend did not reach significance. These findings indicate the utility and feasibility of monitoring cardiovascular risk in a NASH trial. The utility of CAC scores may be higher in trials of longer duration (⩾52 weeks) and with older patients (age ⩾45). ClinicalTrials.gov registration: NCT01766713.
Keywords: Framingham risk; coronary artery calcium; fatty liver; hepatic steatosis; score.
Conflict of interest statement
Figures
References
-
- Agatston A., Janowitz W., Hildner F., Zusmer N., Viamonte M., Jr., Detrano R. (1990) Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15: 827–832. - PubMed
-
- Andrus B., Lacaille D. (2014) 2013 ACC/AHA guideline on the assessment of cardiovascular risk. J Am Coll Cardiol 63: 2886. - PubMed
-
- Arulanandan A., Ang B., Bettencourt R., Hooker J., Behling C., Lin G., et al. (2015) Association between quantity of liver fat and cardiovascular risk in patients with nonalcoholic fatty liver disease independent of nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol 13: 1513–1520. - PubMed
-
- Callister T., Raggi P., Cooil B., Lippolis N., Russo D. (1998) Effect of HMG-COA Reductase inhibitors on coronary artery disease as assessed by electron-beam computed tomography. N Engl J Med 339: 1972–1978. - PubMed
