

A Novel Brief Therapy for Patients Who Attempt Suicide: A 24-months Follow-Up Randomized Controlled Study of the Attempted Suicide Short Intervention Program (ASSIP)
- PMID: 26930055
- PMCID: PMC4773217
- DOI: 10.1371/journal.pmed.1001968
A Novel Brief Therapy for Patients Who Attempt Suicide: A 24-months Follow-Up Randomized Controlled Study of the Attempted Suicide Short Intervention Program (ASSIP)
Abstract
Background: Attempted suicide is the main risk factor for suicide and repeated suicide attempts. However, the evidence for follow-up treatments reducing suicidal behavior in these patients is limited. The objective of the present study was to evaluate the efficacy of the Attempted Suicide Short Intervention Program (ASSIP) in reducing suicidal behavior. ASSIP is a novel brief therapy based on a patient-centered model of suicidal behavior, with an emphasis on early therapeutic alliance.
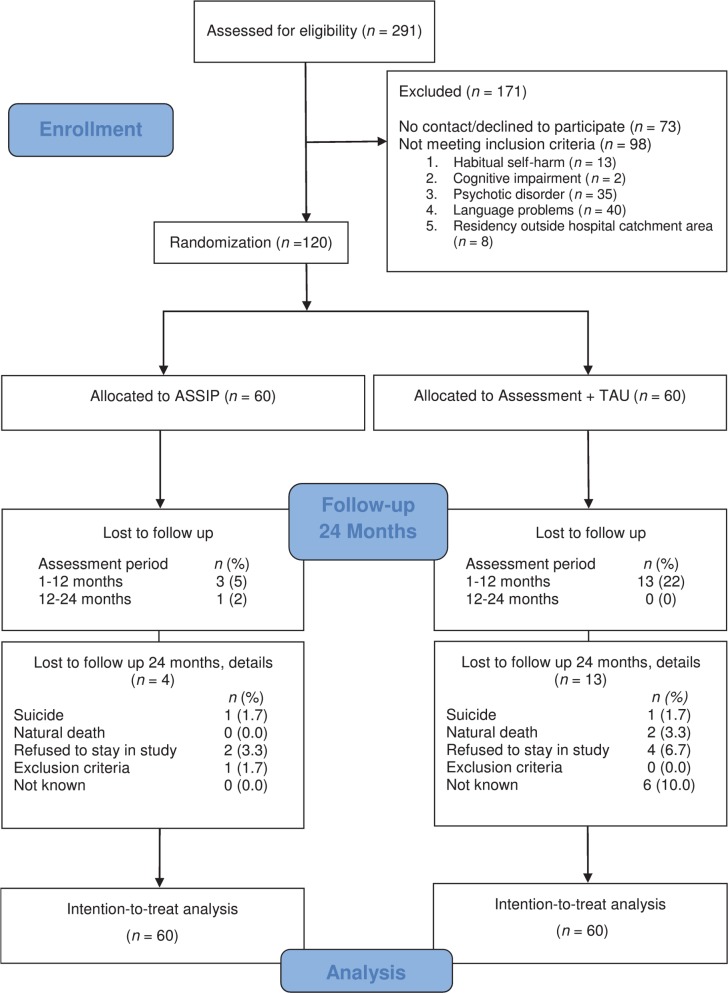
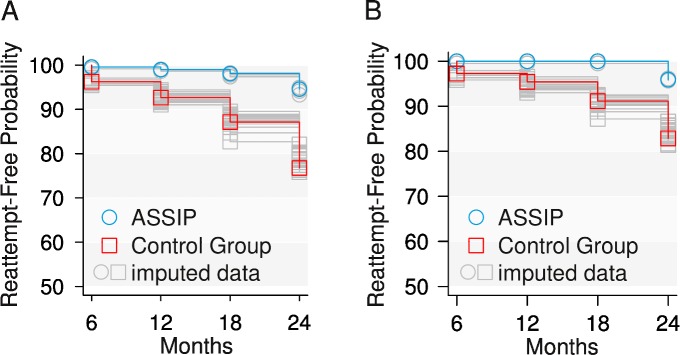
Methods and findings: Patients who had recently attempted suicide were randomly allocated to treatment as usual (n = 60) or treatment as usual plus ASSIP (n = 60). ASSIP participants received three therapy sessions followed by regular contact through personalized letters over 24 months. Participants considered to be at high risk of suicide were included, 63% were diagnosed with an affective disorder, and 50% had a history of prior suicide attempts. Clinical exclusion criteria were habitual self-harm, serious cognitive impairment, and psychotic disorder. Study participants completed a set of psychosocial and clinical questionnaires every 6 months over a 24-month follow-up period. The study represents a real-world clinical setting at an outpatient clinic of a university hospital of psychiatry. The primary outcome measure was repeat suicide attempts during the 24-month follow-up period. Secondary outcome measures were suicidal ideation, depression, and health-care utilization. Furthermore, effects of prior suicide attempts, depression at baseline, diagnosis, and therapeutic alliance on outcome were investigated. During the 24-month follow-up period, five repeat suicide attempts were recorded in the ASSIP group and 41 attempts in the control group. The rates of participants reattempting suicide at least once were 8.3% (n = 5) and 26.7% (n = 16). ASSIP was associated with an approximately 80% reduced risk of participants making at least one repeat suicide attempt (Wald χ21 = 13.1, 95% CI 12.4-13.7, p < 0.001). ASSIP participants spent 72% fewer days in the hospital during follow-up (ASSIP: 29 d; control group: 105 d; W = 94.5, p = 0.038). Higher scores of patient-rated therapeutic alliance in the ASSIP group were associated with a lower rate of repeat suicide attempts. Prior suicide attempts, depression, and a diagnosis of personality disorder at baseline did not significantly affect outcome. Participants with a diagnosis of borderline personality disorder (n = 20) had more previous suicide attempts and a higher number of reattempts. Key study limitations were missing data and dropout rates. Although both were generally low, they increased during follow-up. At 24 months, the group difference in dropout rate was significant: ASSIP, 7% (n = 4); control, 22% (n = 13). A further limitation is that we do not have detailed information of the co-active follow-up treatment apart from participant self-reports every 6 months on the setting and the duration of the co-active treatment.
Conclusions: ASSIP, a manual-based brief therapy for patients who have recently attempted suicide, administered in addition to the usual clinical treatment, was efficacious in reducing suicidal behavior in a real-world clinical setting. ASSIP fulfills the need for an easy-to-administer low-cost intervention. Large pragmatic trials will be needed to conclusively establish the efficacy of ASSIP and replicate our findings in other clinical settings.
Trial registration: ClinicalTrials.gov NCT02505373.
Conflict of interest statement
We have read the journal's policy and the authors of this manuscript have the following competing interests: KM and AGM received royalties from Hogrefe Publishing for "ASSIP—Attempted Suicide Short Intervention Program: A Manual for Clinicians. K. Michel & A. Gysin-Maillart (2015)."
Figures
References
-
- Hoyert DL, Kung H- C, Smith BL. Deaths: preliminary data for 2003. Natl Vital Stat Rep. 2005;53:1–48. - PubMed
-
- Drapeau CW, McIntosh JL. U.S.A. suicide: 2013 official final data Washington (District of Columbia): American Association of Suicidology; 2015.
-
- Substance Abuse and Mental Health Services Administration. The NSDUH report: substance use and mental health estimates from the 2013 national survey on drug use and health—overview of findings Rockville (Maryland): Substance Abuse and Mental Health Services Administration; 2014. - PubMed
-
- National Action Alliance for Suicide Prevention. A prioritized research agenda: an action plan to save lives Rockville (Maryland): National Institute of Mental Health and Research Prioritization Task Force; 2014.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
